
    


|
The CBS News
Space Reporter's Handbook
STS-51L/107 Supplement
Remembering the Final Flights
of
Challenger and Columbia

Written, Compiled and Edited By
William G. Harwood
Aerospace Writer/Consultant
bharwood@earthlink.net
Contents
STS-51L (Challenger) Background
Launch-day Coverage
Rogers Commission Accident Investigation
Rogers Commission Recommendations
Fate of the Crew
Accident Timeline
For more detailed information about Challenger and
flight STS-51L, please see:
http://cbsnews.cbs.com/network/news/space/51Lintro.html
STS-107 (Columbia) Background
Launch-day Coverage
Accident Investigation
Recommendations of the Columbia Accident Investigation
Board
Fate of the Crew
Accident Timeline
STS-51L
The shuttle Challenger, NASA's second manned orbiter, blasted off on its final mission at 11:38 a.m. EST on Jan. 28, 1986. The initial moments of the 25th shuttle flight appeared normal, but just over a minute into flight, Challenger exploded in a terrifying fireball. Here is part of one of the many stories the author wrote that day as Cape Canaveral bureau manager for United Press International (note: breaking news wire service stories are written "on the fly" in real time and readers familiar with Challenger's destruction will spot several inadvertent errors):
NASA says astronauts apparently
dead
By WILLIAM HARWOOD
CAPE CANAVERAL, Fla. (UPI) – The space shuttle Challenger exploded shortly after blastoff today and hurtled into the Atlantic Ocean. The seven crew members, including teacher Christa McAuliffe, apparently were killed in the worst disaster in space history.
"It is a national tragedy," said Jesse Moore, director of the Johnson Space Center. "I regret that I have to report … that searches … did not reveal any evidence that the crew members are alive."
He said data from instruments, launch pad systems and other sources would be impounded for an investigation.
 The
explosion occurred while two powerful booster rockets were still attached to
the shuttle. There was no way for the crew to escape the out-of-control
spacecraft, which fell into the ocean 18 miles off the coast. Burning debris
falling from the sky kept rescuers from reaching the scene immediately.
The
explosion occurred while two powerful booster rockets were still attached to
the shuttle. There was no way for the crew to escape the out-of-control
spacecraft, which fell into the ocean 18 miles off the coast. Burning debris
falling from the sky kept rescuers from reaching the scene immediately.
"We have a report that the vehicle has exploded," said NASA spokesman Steve Nesbitt. "We are now looking at all the contingency operations awaiting word from any recovery forces downrange."
On board the Challenger were commander Francis "Dick" Scobee, co-pilot Michael Smith, Judith Resnik, Ellison Onizuka, Ronald McNair, satellite engineer Gregory Jarvis and McAuliffe, the Concord, N.H. social studies teacher who was chosen from 11,000 candidates to be the first private citizen to fly on a shuttle.
Blow by: In this photo, black smoke can
be seen billowing from an O-ring joint at the base of Challenger's right-side
solid-fuel booster moments after ignition. The joint resealed itself but
eventually reopened, triggering the shuttle's destruction 73 seconds after
liftoff.
Unlike the shuttle Columbia during its first flights at the dawn of the shuttle era, Challenger was not equipped with ejection seats or other ways for the crew to get out of the spacecraft. McAuliffe's parents, Edward and Grace Corrigan, watching from the VIP site three miles from the launch pad, hugged each other and sobbed as the fireball erupted in the sky. Students at her school, assembled to watch their teacher's launch, watched in stunned silence.
Other students, friends and fellow teachers in Concord cheered the blastoff and then fell into stony silence as the disaster was brought home to them on television. Mark Letalien, a junior at the Concord high school, said "I didn't believe it happened. They made such a big thing about it. Everyone's watching her and she gets killed."
It was the 25th shuttle flight, the 10th for Challenger and the worst disaster in the nation's space program. It came exactly 19 years and a day from the only previous accident - aboard the first Apollo moon capsule on its launch pad Jan. 27, 1967. Astronauts Virgil "Gus" Grissom, Edward White and Roger Chaffee died in that fire.
NASA said Challenger's launch appeared entirely normal until one minute and 15 seconds after liftoff, when the shuttle had accelerated to a speed of 1,977 mph, three times the speed of sound. It was 4.9 miles up and 18 miles out over the ocean.
"Challenger, go at throttle up," mission control told the spacecraft 52 seconds after launch. Scobee's final words to mission control were: "Roger, go at throttle up." Television replays showed close-ups of the speeding ship suddenly enveloped in a ball of fire. Its engines continued firing, raising it out of the flames, but it was out of control.
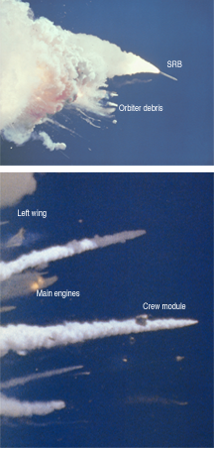
Multiple contrails could be seen streaking through the sky as the $1.1 billion shuttle arced out over the Atlantic and debris fell into the sea.
In Washington, President Reagan was in an Oval Office meeting whe4n aides brought him the grim news. He rushed into a study in time to see a television replay of the explosion. His face was creased with horror and anxiety. The House of Representatives recessed in the face of the national tragedy.
o o
o
A panel of outside experts led by former Secretary of State William Rogers concluded Challenger was destroyed by the rupture of an O-ring joint in the shuttle's right-side solid-fuel booster. The resulting "burn through" created a jet of flame that ultimately ate through Challenger's external tank, triggering its collapse 73 seconds after blastoff. Almost simultaneously, Challenger, traveling faster than sound, broke apart after being subjected to aerodynamic forces it was not designed to withstand. The ship's crew cabin broke away from the rest of the shuttle and crashed into the Atlantic Ocean at more than 200 mph (see photo at left).
The Rogers Commission report was delivered on June 6 to Camp David, Md., where President Reagan was spending the weekend. A formal presentation with the members of the commission was hgeld in the Rose Garden at the White House. The 256-page report was divided into nine chapters. The first two chapters presented a brief history of the shuttle program and past flights and detailed the events leading up to Challenger's launching on Jan. 28. The commission also presented a detailed timeline of the disaster before getting down to business in Chapter 4.
The Cause of the Accident
The Rogers Commission listed 16 findings on the primary cause of the accident before stating the following conclusion:
"The commission concluded that the cause of the Challenger accident was the failure of the pressure seal in the aft field joint of the right Solid Rocket Motor. The failure was due to a faulty design unacceptably sensitive to a number of factors. These factors were the effects of temperature, physical dimensions, the character of materials, the effects of reusability, processing and the reaction of the joint to dynamic loading."
A thorough analysis of all available evidence showed no abnormalities with the external fuel tank, Challenger and its three main engines or the shuttle's payload and records showed all the hardware used in flight 51-L met NASA specifications. Launch processing, from the initial stacking of the rocket boosters to work done at the launch pad was normal, but during assembly of the right-side booster, engineers ran into snags. One of the fuel segments that mated at the aft field joint was severely out of round and had to be forced into the proper shape with a high-power hydraulic tool. In addition, measurements showed that because of previous use, the two fuel segments in question had slightly larger diameters than normal but they still were within specifications.
Recall for a moment the construction of the joint. The upper rim of the bottom fuel segment, called a clevis, is an upward-facing U-shaped groove. The lower rim of the fuel segment above, called a tang, slides into the clevis and the resulting interlocking joint is bolted together with 177 high-strength steel pins. Running around the interior of the inner leg of the clevis are the two rubber O-ring seals. Because of the larger than normal joint diameters, at the moment of ignition, the tang and clevis had an average gap of .004 inches, which would have compressed the O-rings severely. Because the fuel segments were slightly out of round, the smallest gap was in the area where the rupture occurred during flight, although it is not known if the high compression on the O-ring was present at liftoff.
 It
was a record 36 degrees when Challenger took off and infrared measurements
taken at the launch pad showed the temperature around the circumference of the
aft field joint was in the neighborhood of 28 degrees in the area where the
rupture occurred, the coldest spot on the booster. To understand the
significance of the temperature factor, consider again the operation of the
rocket motor at ignition when internal pressure shoots from zero to nearly
1,000 pounds per square inch. This tremendous force pushes outward and causes
the joints to bulge slightly, a phenomenon known as joint rotation. During the
ignition transient, the tang and clevis typically separate as much as .017 and
.029 inches where the primary and secondary O-rings are located. The gap
opening reaches maximum about 600 milliseconds after ignition when the motor
reaches full pressure. To keep the joint sealed as the tang-clevis separation
increases during ignition, the O-rings must seat properly and the commission
said cold O-rings take longer to reach the proper position.
It
was a record 36 degrees when Challenger took off and infrared measurements
taken at the launch pad showed the temperature around the circumference of the
aft field joint was in the neighborhood of 28 degrees in the area where the
rupture occurred, the coldest spot on the booster. To understand the
significance of the temperature factor, consider again the operation of the
rocket motor at ignition when internal pressure shoots from zero to nearly
1,000 pounds per square inch. This tremendous force pushes outward and causes
the joints to bulge slightly, a phenomenon known as joint rotation. During the
ignition transient, the tang and clevis typically separate as much as .017 and
.029 inches where the primary and secondary O-rings are located. The gap
opening reaches maximum about 600 milliseconds after ignition when the motor
reaches full pressure. To keep the joint sealed as the tang-clevis separation
increases during ignition, the O-rings must seat properly and the commission
said cold O-rings take longer to reach the proper position.
"At the cold launch temperature experienced, the O-ring would be very slow in returning to its normal rounded shape. It would not follow the opening of the tang-to-clevis gap. It would remain in its compressed position in the O-ring channel and not provide a space between itself and the upstream channel wall. Thus, it is probable the O-ring would not be pressure actuated to seal the gap in time to preclude joint failure due to blow-by and erosion from hot combustion gases," the report said.
Further, the commission found that experimental evidence showed other factors, such as humidity and the performance of the heat-shielding putty in the joint "can delay pressure application to the joint by 500 milliseconds or more." Records showed that in each shuttle launch in temperature below 61 degrees, one or more booster O-rings showed signs of erosion or the effects of heat. Complicating the picture, there was the possibility of ice in the suspect joint because Challenger had been exposed to seven inches of rainfall during its month on the launch pad prior to blastoff. Research showed ice could have prevented proper sealing by the secondary O-ring.
Launch pad cameras showed puffs of black smoke shooting from the region of the aft field joint beginning about the same time the motor reached full pressure. The commission said two overall failure scenarios were possible: a small leak could have developed at ignition that slowly grew to the point that flame erupted through the joint as photographs indicated some 58 seconds after blastoff. More likely, however, the gap between the burned O-rings and the clevis probably was sealed up by "deposition of a fragile buildup of aluminum oxide and other combustion debris. The resealed section of the joint could have been disturbed by thrust vectoring (steering), space shuttle motion and flight loads induced by changing winds aloft." NASA revealed after the accident that wind shear was higher for Challenger's mission than for any previous shuttle flight.
That the shuttle booster joints were faulty and overly dependent on a variety of factors was clear. The commission's findings on the secondary causes of the disaster were more subtle but just as damning to the space agency.
The Contributing Cause of the Accident
"The decision to launch the Challenger was flawed," the Rogers Commission said. "Those who made that decision were unaware of the recent history of problems concerning the O-rings and the joint and were unaware of the initial written recommendation of the contractor advising against the launch at temperatures below 53 degrees Fahrenheit and the continuing opposition of the engineers at Thiokol after the management reversed its position. They did not have a clear understanding of Rockwell's concern that it was not safe to launch because of ice on the pad. If the decision makers had known all of the facts, it is highly unlikely that they would have decided to launch 51-L on January 28, 1986."
Before shuttles are cleared for flight, a formal "flight readiness review" is held by top NASA managers to discuss any open items that might affect a launch. Previous flights are reviewed to make sure any problems had been addressed before commiting the next shuttle for launch. Mulloy testified NASA management was well aware of the O-ring issue and cited the flight readiness review record as proof. He was correct in that during several preceding flight readiness reviews, the O-ring problem was mentioned. But it was only mentioned in the context that it was an acceptable risk and that the boosters had plenty of margin. It was not mentioned at all during the 51-L readiness review.
"It is disturbing to the commission that contrary to the testimony of the solid rocket booster project manager, the seriousness of concern was not conveyed in Flight Readiness Review to Level 1 and the 51-L readiness review was silent."
Keel said later the real turning point in the commission investigation came on Feb. 10 during a closed hearing in Washington. It was there the commission learned of the launch-eve debate over clearing Challenger for launch. Boisjoly would later recall the events of Jan. 27 in this manner:
Boisjoly: "I felt personally that management was under a lot of pressure to launch and that they made a very tough decision, but I didn't agree with it. One of my colleagues that was in the meeting summed it up best. This was a meeting where the determination was to launch and it was up to us to prove beyond a shadow of a doubt that it was not safe to do so. This is in total reverse to what the position usually is in a preflight conversation or a flight readiness review. It is usually exactly opposite that."
Commission member Arthur B.C. Walker: "Do you know the source of the pressure on management that you alluded to?"
Boisjoly: "Well, the comments made over the [teleconference network] is what I felt, I can't speak for them, but I felt it, I felt the tone of the meeting exactly as I summed up, that we were being put in a position to prove that we should not launch rather then being put in the position and prove that we had enough data for launch. And I felt that very real."
The Rogers Commission concluded that a "well structured" management system with the emphasis on flight safety would have elevated the booster O-ring issue to the status it deserved and that NASA's decision-making process was clearly faulty. One can only wonder how many other launch-eve debates occurred during the previous 24 missions that were never mentioned because the flight turned out to be a success.
"Had these matters been clearly stated and emphasized in the flight readiness process in terms reflecting the views of most of the Thiokol engineers and at least some of the Marshall engineers, it seems likely that the launch of 51-L might not have occurred when it did," the commission said.
The commission also determined that the waiving of launch constraints based on previous success came at the expense of flight safety because the waivers did not necessarily reach top-level management for a decision. Finally, the commission charged engineers at the Marshall Space Flight Center where the booster program was managed had a "propensity" for keeping knowledge of potentially serious problems away from other field centers in a bid to address them internally.
An Accident Rooted in History
"The Space Shuttle's Solid Rocket Booster problem began with the faulty design of its joint and increased as both NASA and contractor management first failed to recognize it as a problem, then failed to fix it and finally treated it as an acceptable flight risk," the Rogers Commission said.
Morton Thiokol won the contract to build shuttle boosters in 1973. Of the four competitors, Thiokol ranked at the bottom for design and development but came in first in the management category. NASA later said Thiokol was selected because "cost advantages were substantial and consistent throughout all areas evaluated." The result was an $800 million cost-plus-award-fee contract.
Morton Thiokol hoped to keep costs down by borrowing heavily from the design of the Titan 3 solid rocket motors. Both systems, for example, used tang and clevis joints but the shuttle design had major differences as well. Unlike in the Titan, which relied on a single O-ring seal, two rubber O-rings were employed in the shuttle booster and both faced heavy pressure loads at launch. The way the seals worked in the shuttle boosters was elegant in its simplicity. Before fuel joints were to be mated, an asbestos-filled putty would be used to fill in the gap between the two propellant faces of the fuel segments. The putty, then, would serve as a barrier to prevent hot gas from reaching the O-ring seals. But the putty was plastic so when the rocket was ignited, internal pressure would force the putty to flow toward the outside of the joint. In doing so, air between the putty and the O-ring would become pressurized, forcing the O-ring to "extrude" into the minute gap between the clevis and tang. In this manner, the joint would be sealed and even if the primary O-ring failed to operate, the secondary seal would fill in the gap, so to speak. To make sure the O-rings were, in fact, able to seal the joints prior to ignition, Thiokol included a "leak test port" in each booster joint. Once assembled, the space between the two O-rings could be pressurized with 50 psi air. If the pressure stayed steady, engineers would know the joint was airtight and that no path from the propellant to the primary O-ring existed for hot gas or flame.
So much for theory. When testing began, results were not what Thiokol engineers expected.
The design of the joint had led engineers to believe that once pressurized, the gap between the tang and clevis actually would decrease slightly, thereby improving the sealing action of the O-rings. To test the booster's structural integrity, Thiokol conducted "hydroburst" tests in 1977. In these tests, water was pumped inside a booster case and pressurized to 1.5 times actual operating pressure. Careful measurements were made and to their surprise, engineers realized that the tang and clevis joint actually bulged outward, widening the gap between the joint members. While Thiokol tended to downplay the significance of the finding at the time, engineers at Marshall were dismayed by the results. John Q. Miller, a chief booster engineer at the Alabama rocket center, wrote a memo on Jan. 9, 1978, to his superiors, saying, "We see no valid reason for not designing to accepted standards" and that improvements were mandatory "to prevent hot gas leaks and resulting catastrophic failure." This memo and another along the same lines actually were authored by Leon Ray, a Marshall engineer, with Miller's agreement. Other memos followed but the Rogers Commission said Thiokol officials never received copies. In any case, the Thiokol booster design passed its Phase 1 certification review in March 1979. Meanwhile, ground test firings confirmed the clevis-tang gap opening. An independent oversight committee also said pressurization through the leak test port pushed the primary O-ring the wrong way so that when the motor was ignited, the compression from burning propellant had to push the O-ring over its groove in order for it to extrude into the clevis-tang gap. Still, NASA engineers at Marshall concluded "safety factors to be adequate for the current design" and that the secondary O-ring would serve as a redundant backup throughout flight.
On Sept. 15, 1980, the solid rocket booster joints were classified as criticality 1R, meaning the system was redundant because of the secondary O-ring. Even so, the wording of the critical items list left much room for doubt: "Redundancy of the secondary field joint seal cannot be verified after motor case pressure reaches approximately 40 percent of maximum expected operating pressure." The joint was classified as criticality 1R until December 1982 when it was changed to criticality 1. Two events prompted the change: the switch to a non-asbestos insulating putty - the original manufacturer had discontinued production - and the results of tests in May 1982 that finally convinced Marshall management that the secondary O-ring would not function after motor pressurization. Criticality 1 systems are defined as those in which a single failure results in loss of mission, vehicle and crew. Even though the classification was changed, NASA engineers and their counterparts at Morton Thiokol still considered the joint redundant through the ignition transient. The Rogers Commission found this to be a fatal flaw in judgment.
Criticality 1 systems must receive a formal "waiver" to allow flight. On March 28, 1983, Michael Weeks, associate administrator for space flight (technical) signed the document that allowed continued shuttle missions despite the joint concerns.
"We felt at the time, all of the people in the program I think felt that this solid rocket motor in particular ... was probably one of the least worrisome things we had in the program," Weeks said.
Then came the flight of mission 41-B, the 10th shuttle mission, launched Feb. 3, 1984. Prior to that time, only two flights had experienced O-ring damage: the second shuttle mission and the sixth. In both cases, only a single joint was involved. But after 41-B, inspectors found damage to a field joint and a nozzle joint. Marshall engineers were concerned about the unexpected damage, but a problem assessment report concluded: "This is not a constraint to future launches." For the next shuttle flight, 41-C, NASA managers were advised launch should be approved but that there was a possibility of some O-ring erosion. Meanwhile, to make absolutely sure the O-rings were seated properly prior to launch, the leak test pressure was increased to 100 psi and later to 200 psi, even though Marshall engineers realized that increased the possibility of creating blow holes through the insulating putty. Such blow holes, in turn, could provide paths for hot gas to reach the O-rings. In any case, the statistics are simple: of the first nine shuttle flights, when joints were tested with 50 psi or 100 psi pressure, only one field joint problem was noticed. With the 200 psi tests, more than 50 percent of the shuttle missions exhibited some field joint O-ring erosion.
So even though research was underway to improve the joint design, shuttles continued flying. On Jan. 24, 1985, Discovery took off on the first classified military shuttle mission, flight 51-C. The temperature at launch time was a record 53 degrees and O-ring erosion was noted in both boosters after recovery. Damage was extensive: both booster nozzle primary O-rings showed signs of blow by during ignition and both the primary and secondary seals in the right booster's center segment field joint were affected by heat. Thiokol engineers would later say temperature apparently increased the chances for O-ring damage or erosion by reducing resiliency. Concern mounted after the flight of mission 51-B in April 1985 when engineers discovered a nozzle primary O-ring had been damaged and failed to seat at all and that the secondary seal also was eroded. This was serious and more studies were ordered. Mulloy then instituted a launch constraint, meaning a waiver was required before every succeeding mission. Mulloy signed such waivers six flights in a row before Challenger took off for the last time.
On Aug. 19, 1985, NASA managers in Washington were briefed on the O-ring issue and the next day, Morton Thiokol established an O-ring task force because "the result of a leak at any of the joints would be catastrophic." But company engineers told the commission the task force ran into red tape and a lack of cooperation.
"The genesis of the Challenger accident - the failure of the joint of the right solid rocket motor - began with decisions made in the design of the joint and in the failure by both Thiokol and NASA's solid rocket booster project office to understand and respond to facts obtained during testing," the Rogers Commission concluded.
The panel said NASA's testing program was inadequate, that engineers never had a good understanding of the mechanics of joint sealing and that the material presented to NASA management in August 1985 "was sufficiently detailed to require corrective action prior to the next flight."
Pressures on the System
"With the 1982 completion of the orbital test flight series, NASA began a planned acceleration of the Space Shuttle launch schedule," the Rogers Commission said. "One early plan contemplated an eventual rate of a mission a week, but realism forced several downward revisions. In 1985, NASA published a projection calling for an annual rate of 24 flights by 1990. Long before the Challenger accident, however, it was becoming obvious that even the modified goal of two flights a month was overambitious."
When the shuttle program was conceived, it was hailed as the answer to the high cost of space flight. By building a reusable space vehicle, the United States would be able to lower the cost of placing a payload into orbit while at the same time, increase its operational capability on the high frontier. The nation's space policy then focused on the shuttle as the premier launcher in the American inventory and expendable rockets were phased out. Once shuttle flights began, NASA quickly fell under pressure to meet a heavy schedule of satellite launches for commercial, military and scientific endeavors. And as the flight rate increased, the space agency's resources became stretched to the limit. Indeed, the Rogers Commission said evidence indicated even if the 51-L disaster had been avoided, NASA would have been unable to meet the 16-launch schedule planned for 1986.
But NASA's can-do attitude refused to let the agency admit its own limitations as it struggled along against increasingly significant odds and diminishing resources. The Rogers Commission found that astronaut training time was being cut back, that frequent and late payload changes disrupted flight planning and that a lack of spare parts was beginning to manifest itself in flight impacts at the time of the Challenger accident.
The Rogers Commission concluded:
1. "The capabilities of the system were stretched to the limit to support the flight rate in winter 1985/1986," the commission wrote. "Projections into the spring and summer of 1986 showed a clear trend; the system, as it existed, would have been unable to deliver crew training software for scheduled flights by the designated dates. The result would have been an unacceptable compression of the time available for the crews to accomplish their required training.
2. "Spare parts are in short supply. The shuttle program made a conscious decision to postpone spare parts procurements in favor of budget items of perceived higher priority. Lack of spare parts would likely have limited flight operations in 1986.
3. "Stated manifesting policies [rules governing payload assignments] are not enforced. Numerous late manifest changes (after the cargo integration review) have been made to both major payloads and minor payloads throughout the shuttle program.
4. "The scheduled flight rate did not accurately reflect the capabilities and resources.
5. "Training simulators may be the limiting factor on the flight rate; the two current simulators cannot train crews for more than 12-15 flights per year.
6. "When flights come in rapid succession, current requirements do not ensure that critical anomalies occurring during one flight are identified and addressed appropriately before the next flight."
Other Safety Considerations
The Rogers Commission also identified a number of safety considerations to be addressed by NASA before the resumption of shuttle flights. The realization that Challenger's crew had no survivable abort options during solid rocket flight prompted the commission to recommend a re-evaluation of all possible abort schemes and escape options.
Two types of shuttle aborts were possible at the time of the Challenger accident: the four intact aborts, in which the shuttle crew attempts an emergency landing on a runway, and contingency aborts, in which the shuttle is not able to make it to a runway and instead "ditches" in the ocean. But the commission said tests at NASA's Langely Research Center showed an impact in the ocean probably would cause major structural damage to the orbiter's crew cabin. In addition, "payloads in the cargo bay are not designed to withstand decelerations as high as those expected and would very possibly break free and travel forward into the crew cabin." Not a pleasant prospect.
"My feeling is so strong that the orbiter will not survive a ditching, and that includes land, water or any unprepared surface," astronaut Weitz told the commission. "I think if we put the crew in a position where they're going to be asked to do a contingency abort, then they need some means to get out of the vehicle before it contacts earth."
If there was a clear "winner" in the Rogers Commission report is was the astronauts. Nearly every concern raised by Young and his colleagues was addressed and NASA managers privately grumbled that with the re-emergence of "astronaut power," the agency would become so conservative it would be next to impossible to get a shuttle off the ground.
Recommendations:
The Rogers Commission made nine recommendations to conclude its investigation of the worst disaster in space history.
1. A complete redesign of the solid rocket booster segment joints was required with the emphasis on gaining a complete understanding of the mechanics of seal operation; the joints should be as structurally stiff as the walls of the rockets and thus less susceptible to rotation; and NASA should consider vertical test firings to ensure duplication of the loads experienced during a shuttle launch. In addition, the panel recommended that NASA ask the National Research Council to set up an independent review committee to oversee the redesign of the booster joints.
2. NASA's shuttle program management system should be reviewed and restructured, with the program manger given more direct control over operations, and NASA should "encourage the transition of qualified astronauts into agency management positions" to utilize their flight experience and to ensure proper attention is paid to flight safety. In addition, the commission said NASA should establish a shuttle safety advisory panel.
3. The commission recommended a complete review of all criticality 1, 1R, 2 and 2R systems before resumption of shuttle flights.
4. NASA was told to set up an office of Safety, Reliability and Quality Control under an associate administrator reporting to the administrator of the space agency. This office would operate autonomously and have oversight responsibilities for all NASA programs.
5. Communications should be improved to make sure critical information about shuttle systems makes it from the lowest level engineer to the top managers in the program. "The commission found that Marshall Space Flight Center project managers, because of a tendency at Marshall to management isolation, failed to provide full and timely information bearing on the safety of flight 51-L to other vital elements of shuttle program management," the panel said. Astronauts should participate in flight readiness reviews, which should be recorded, and new policies should be developed to "govern the imposition and removal of shuttle launch constraints."
6. NASA should take action to improve safety during shuttle landings by improving the shuttle's brakes, tires and steering system and terminating missions at Edwards Air Force Base, Calif., until weather forecasting improvements are made at the Kennedy Space Center.
7. "The commission recommends that NASA make all efforts to provide a crew escape system for use during controlled gliding flight." In addition, NASA was told to "make every effort" to develop software modifications that would allow an intact landing even in the event of multiple engine failures early in flight.
8. Pressure to maintain an overly ambitious flight rate played a role in the Challenger disaster and the Rogers Commission recommended development of new expendable rockets to augment the shuttle fleet.
9. "Installation, test and maintenance procedures must be especially rigorous for space shuttle items designated criticality 1. NASA should establish a system of analyzing and reporting performance trends in such items." In addition, the commission told NASA to end its practice of cannibalizing parts from one orbiter to keep another flying and instead to restore a healthy spare parts program despite the cost.
o o
o
Along with redesigning the O-ring booster joints, the agency reviewed the status of the overall shuttle program and ordered hundreds of modifications and improvements to beef up the safety of the shuttle itself. The shuttle "critical items list," which ranks systems and components according to the results of a failure, underwent a thorough review with far-reaching results. Criticality 1 components are those in which a failure leads to loss of vehicle and crew while criticality 1R systems are those in which a redundant backup is in place. Before the Challenger disaster, NASA listed 617 criticality 1 and 787 criticality 1R systems, a total of 1,404. As a result of the post-Challenger review, 1,514 criticality 1 systems were identified along with 2,113 criticality 1R components, a total of 3,627.
The numbers increased because NASA took a much harder look at the shuttle and its systems in the wake of Challenger and while at first glance they would appear to imply the shuttle is more dangerous than before, in reality they mean NASA simply has a better, more realistic understanding of the ship.
In the shuttle itself, more than 210 changes were ordered for first flight along with about 30 to widen safety margins in the powerful hydrogen-fueled main engines by improving welds and reducing bearing wear and turbine blade cracks, a source of concern in the past. Among the shuttle modifications were landing gear brake improvements and a redesign of the 17-inch valves in the main engine propellant feed lines to prevent premature closure and inadvertent engine shutdown.
Other major changes include installation of ribs to strengthen the structure of the shuttle's airframe, an automatic cutoff system to prevent maneuvering rocket problems and modifications to improve the ability of the nose section of the shuttle to withstand the tremendous heat of atmospheric re-entry. About 100 changes were made in the computer programs that actually fly the shuttle to take into account the performance of modified hardware and to improve safety margins.
NASA re-emphasized safety in mission design, implementing stricter weather criteria, new launch commit criteria and a revamped management structure that gave the final responsibility for clearing a shuttle for launch to an astronaut.

Challenger's crew: Back row, left to
right: Ellison Onizuka, Christa McAuliffe,
Greg Jarvis, Judy Resnik; Front row,
left to right: Mike Smith, Dick Scobee, Ron McNair
Shuttle flights resumed Sept. 29, 1988, and NASA launched 87 successful flights in a row before Columbia returned to Earth on Feb. 1, 2003.
o o
o
The Fate of Challenger's Crew
"NASA is unable to determine positively the cause of death of the Challenger astronauts but has established that it is possible, but not certain, that loss of consciousness did occur in the seconds following the orbiter breakup." NASA Press Release
"We have now turned our full efforts to the future, but will never forget our seven friends who gave their lives to America's space frontier." - Rear Adm. Richard Truly, Associate Administrator for Space Flight
The Rogers Commission did not discuss the fate of the crew or provide much detail about the crew cabin wreckage. Indeed, all references to "contact 67," the crash site of the crew compartment, were deleted from the official record, including charts that mapped various debris areas. This was done, perhaps, to preclude the possibility that anyone could find out the latitude and longitude of the cabin wreck site for diving and personal salvage. But ultimately, it was simply an extension of NASA's policy of no comment when it came to the astronauts. After all, hundreds of reporters knew the exact coordinates by eavesdropping on Navy radio. In any case, while the astronauts were not discussed in the commission report, the crew module was.
Analysis of crew cabin wreckage indicates the shuttle's windows may have survived the explosion. It is thus possible the crew did not experience high altitude decompression. If so, some or all of the astronauts may have been alive and conscious all the way to impact in the Atlantic some 18 miles northeast of the launch pad. The cabin hit the water at better than 200 mph on Scobee's side. The metal posts of the two forward flight deck seats, for example, were bent sharply to the right by force of impact when the cabin disintegrated.
"The internal crew module components recovered were crushed and distorted, but showed no evidence of heat or fire," the commission report said. "A general consistency among the components was a shear deformation from the top of the components toward the +Y (to the right) direction from a force acting from the left. Components crushed or sheared in the above manner included avionics boxes from all three avionics bays, crew lockers, instrument panels and the seat frames from the commander and the pilot. The more extensive and heavier crush damage appeared on components nearer the upper left side of the crew module. The magnitude and direction of the crush damage indicates that the module was in a nose down and steep left bank attitude when it hit the water.
"The fact that pieces of forward fuselage upper shell were recovered with the crew module indicates that the upper shell remained attached to the crew module until water impact. Pieces of upper forward fuselage shell recovered or found with the crew module included cockpit window frames, the ingress/egress hatch, structure around the hatch frame and pieces of the left and right sides. The window glass from all of the windows, including the hatch window, was fractured with only fragments of glass remaining in the frames."
Several large objects were tracked by radar after the shuttle disintegrated. One such object, classified as "Object D," hit the water 207 seconds after launch about 18 nautical miles east of launch pad 39B. This apparently was the crew cabin. "It left no trail and had a bright white appearance (black and white recording) until about T+175 seconds," an appendix to the Rogers Commission report said. "The image then showed flashes of both white and black until T+187 seconds, after which time it was consistently black. The physical extent of the object was estimated from the TV recording to be about 5 meters." This description is consistent with a slowly spinning crew module, which had black heat-shield tiles on its bottom with white tiles on its side and top.
The largest piece of crew cabin wreckage recovered was a huge chunk of the aft bulkhead containing the airlock hatch that led into the payload bay and one of the two flight deck windows that looked out over the cargo hold. The bulkhead wreckage measured 12 feet by 17 feet.
Here is a chronology of the crew cabin recovery operation and the efforts to determine the fate of the astronauts:
Mid-March Four astronaut "personal egress air packs," called PEAPs, are recovered along with other cabin wreckage.
April 18 NASA announced the crew cabin recovery operation was complete and that identifiable remains of all seven astronauts were on shore undergoing analysis.
April 25 The Armed Forces Institute of Pathology notified NASA it had been unable to determine a cause of death from analysis of remains. Joseph Kerwin, director of life sciences at the Johnson Space Center, began an in-depth analysis of the wreckage in a search for the answer.
May 20 Johnson Space Center crew systems personnel began analysis of the four PEAPs, emergency air packs designed for use if a shuttle crew must attempt an emergency exit on the ground when dangerous vapors might be in the area.
May 21 Investigators found evidence some of the PEAPs had been activated.
June 4 Investigators determined PEAP activation was not caused by crew cabin impact in the ocean.
June 9 Smith's PEAP was identified by serial number.
June 25 The PEAPs were sent to th Army Depot in Corpus Christi, Texas, for further analysis.
June 27 Scobee's PEAP was identified by serial number; Army investigators determined that three of the four air packs had been activated.
July 18 Truly received Kerwin's preliminary report on the fate of the astronauts. On July 24, NASA began informing the astronauts' families about what the investigation had found.
Some of the first wreckage recovered included four flight computers and both the cabin's operational flight recorders, used to record data about various shuttle systems and also used for the cabin's intercom system. It was on this tape that NASA heard Smith say "Uh oh" an instant before the shuttle broke apart, showing that at least some of the astronauts had a brief moment of awareness before the explosion that would claim their lives. On July 28, six months to the day after the disaster, NASA staged a news conference in Washington to discuss the investigation. Kerwin said the cause and time of death remained unknown.
"The findings are inconclusive," he wrote in a letter to Truly. "The impact of the crew compartment with the ocean surface was so violent that evidence of damage occurring in the seconds which followed the explosion was masked. Our final conclusions are:
The cause of death of the Challenger astronauts cannot be positively determined;
The forces to which the crew were exposed during orbiter breakup were probably not sufficient to cause death or serious injury; and
The crew possibly, but not certainly, lost consciousness in the seconds following orbiter breakup due to in-flight loss of crew module pressure."
Accelerometers, instruments that measure the magnitude and direction of forces acting on the shuttle during flight, lost power when the nose section ripped away two tenths of a second after structural break up began. Independent analysis of all recovered data and wreckage concluded the nose pitched down as soon as it broke away and then slowed rapidly from aerodynamic forces. Calculations and analysis of launch photography indicate the acceleration forces the astronauts felt were between 12 and 20 times the force of gravity in a vertical direction, that is, as the cabin broke away, the astronauts were violently pushed down in their seats.
"These accelerations were quite brief," Kerwin wrote. "In two seconds, they were below four G's; in less than 10 seconds, the crew compartment was essentially in free fall. Medical analysis indicates that these accelerations are survivable, and that the probability of major injury to crew members is low."
When Challenger broke up, it was traveling at 1.9 times the speed of sound at an altitude of 48,000 feet. The crew module continued flying upward for some 25 seconds to an altitude of about 65,000 feet before beginning the long fall to the ocean. From breakup to impact took two minutes and 45 seconds. Impact velocity was 207 mph, subjecting the module to a braking force of approximately 200 times the force of gravity. Any astronaut still alive at that moment was killed instantly.
When the cabin ripped away from the fuselage, the crew's oxygen supplies were left behind in the payload bay, "except for a few seconds supply in the lines," Kerwin said. But each astronaut's airtight flight helmet also was connected to a PEAP that contained about six minutes of breathing air. Kerwin said because of the design of the activation switch, it was highly unlikely the PEAPs were turned on by impact. But unlike the oxygen system, the PEAPs did not provide pressurized air and if the cabin lost pressure, they would not have allowed the crew to remain conscious.
"It is possible, but not certain, that the crew lost consciousness due to an in-flight loss of crew module pressure," Kerwin wrote. "Data to support this is:
The accident happened at 48,000 feet and the crew cabin was at that altitude or higher for almost a minute. At that altitude, without an oxygen supply, loss of cabin pressure would have caused rapid loss of consciousness and it would not have been regained before water impact.
PEAP activation could have been an instinctive response to unexpected loss of cabin pressure.
If a leak developed in the crew compartment as a result of structural damage during or after breakup (even if the PEAPs had been activated), the breathing air available would not have prevented rapid loss of consciousness.
The crew seats and restraint harnesses showed patterns of failure which demonstrates that all the seats were in place and occupied at water impact with all harnesses locked. This would likely be the case had rapid loss of consciousness occurred, but it does not constitute proof."
Despite NASA's best efforts, engineers were never able to determine if cabin pressure was lost. Astronaut Crippen said later he was convinced it did, however, because had the cabin maintained pressure there would have been no need to activate the PEAPs. He said in his view, the astronauts made a "desperate" attempt to survive by activating the PEAPs when pressure was suddenly lost.
Of the four PEAPs recovered, the one that belonged to Scobee had not been activated. Of the other three, one was identified as Smith's and because of the location of the activation switch on the back of his seat, Truly said he believed Resnik or Onizuka turned the pilot's emergency air supply on in a heroic bid to save his life. The exact sequence of events will never be known.
Timeline of Challenger's Final Flight
This timeline, assembled by
William Harwood and Rob Navias when both worked for United Press International,
was assembled from telemetry beamed down from the shuttle, recordings made of
the mission control voice command circuits, the NASA-Select audio circuit and
the intercom transcript (times given in seconds after launch at 11:38 a.m. EST,
Jan. 28, 1986).
0.000 - Solid rocket
ignition command is sent.
Resnik, intercom:
"Aaall Riight!"
0.008 - First of eight
25-inch-long, 7-inch-wide exploding bolts fire, four at the base of each
booster, freeing Challenger from launch pad.
0.250 - First continuous
vertical motion is recorded.
0.678 - Film developed
later shows the first evidence of abnormal black smoke appearing slightly above
the suspect joint in Challenger's right-hand solid rocket booster.
0.836 - The black smoke
appears darkest; jets in puffs of three per second, roughly matching harmonic
characteristics of the shuttle vehicle at launch, characteristics directly
related to the energy stored in the shuttle structure by the twang phenomenon
and released as the spacecraft is freed from the launch stand.
0.890 - Ground launch
sequencer computers begin post-liftoff "safing" of launch pad
structures and equipment.
1.000 - Smith, intercom:
"Here we go."
2.733 - Last positive
evidence of smoke above the aft attach fitting that holds the rear of the
right-side booster to the external fuel tank. The aft attach fitting is a
little less than two feet above the fuel segment joint.
3.375 - Last positive
visual indication of smoke swirling under the bottom of the external fuel tank.
Launch commentator Harris
(continuing) "... Liftoff of the 25th space shuttle mission, and it has
cleared the tower."
4.339 - The three
liquid-fueled main engines throttle up from 90 percent thrust to 104 percent
thrust as planned. The capability for 104-percent performance is the result of
improvements made in main engine systems over the decade they were in
development.
5.000 - Data processing
systems (DPS) engineer Andrew Algate, mission control, Houston: "Liftoff confirmed."
Flight director Jay Greene,
Houston: "Liftoff..."
5.000 - Loss of data from
the shuttle at NASA's Merritt Island antenna complex for four data frames. Four
more "data BIT synch dropouts" occur in the next one minute and six
seconds. These are normal and are caused by flame and objects on the horizon
that attenuate radio signals.
5.615 - The backup flight
system computer aboard Challenger commands the S-band PM (phase modulated) and
S-band FM radio systems to switch antennas to maintain communications during
the upcoming roll maneuver.
5.674 - Internal pressure
in the right-side booster is recorded as 11.8 pounds per square inch higher
than normal.
7.724 - The shuttle clears
the launch pad tower and begins a maneuver to roll over, putting the crew in a
"heads down" position below the external tank.
8.000 - Scobee,
air-to-ground: "Houston, Challenger. Roll program."
10.000 - Covey, mission
control: "Roger roll, Challenger."
Flight dynamics officer
(FIDO) Brian Perry, mission control: "Good roll, flight."
Greene: "Rog, good
roll."
11.000 - Smith, intercom:
"Go you mother."
12.000 - Another antenna
switch is ordered to transfer data to the Ponce De Leon tracking station.
14.000 - Resnik, intercom:
"LVLH." Resnik is reminding Scobee and Smith about proper cockpit
switch configurations. "LVLH" is an acronym that stands for
"local vertical, local horizontal."
15.000 - Resnik, intercom:
"(Expletive) hot."
Scobee: "OK."
16.000 - Mission Control
spokesman Nesbitt in Houston: "Good roll program confirmed. Challenger now
heading downrange."
19.000 - Smith, intercom:
"Looks like we've got a lot of wind here today."
Scobee: "Yeah."
19.859 - Challenger's three
main engines receive commands to begin throttling down to 94 percent power, as
planned.
21.124 - The roll maneuver
is completed and Challenger is on the proper trajectory.
21.604 - Right hand SRB
thrust decreases before shuttle reaches maximum dynamic pressure. This is
accomplished by the burn down of ridges in the solid propellant of the forward
fuel segment. Thrust is a function of surface area of propellant burning.
22.000 - Scobee, intercom:
"It's a little hard to see out my window here."
22.204 - Left hand SRB
thrust decreases as planned.
27.000 - Booster systems
engineer (Booster) Jerry Borrer,
mission control: "Throttle down to 94."
Greene: "Ninety
four..."
28.000 - Smith, intercom:
"There's 10,000 feet and Mach point five." The shuttle is 10,000 feet
high traveling at half the speed of sound.
Nesbitt: "Engines
beginning throttling down, now at 94 percent. Normal throttle (setting) for
most of the flight is 104 percent. We'll throttle down to 65 percent shortly.
35.000 - Scobee, intercom:
"Point nine."
35.379 - The three main
engines begin throttling down to 65 percent thrust to reduce acceleration as
aerodynamic pressure builds up.
36.990 - Telemetry data
shows the shuttle's computer system responds properly to wind shear to adjust
the ship's flight path.
40.000 - Smith, intercom:
"There's Mach 1."
Scobee: "Going through
19,000."
43.000 - Scobee, intercom:
"OK, we're throttling down."
45.000 - Nesbitt:
"Engines are at 65 percent. Three engines running normally..."
45.217 - A flash is
observed downstream of the shuttle's right wing.
48.118 - A second flash is
seen trailing the right wing.
48.418 - A third
unexplained flash is seen downstream of the shuttle's right-hand wing. 70 mm
tracking camera closeup: brilliant orange ball of flame, apparently, emerges
from under the right wing and quickly merges with the plume of the solid rocket
boosters. This phenomenon, observed during analysis of tracking film after
launch, has been seen on previous launches but has never been explained.
48.900 - Booster engineer
(Borrer): "Three at 65."
Nesbitt: "... Three
good fuel cells. Three good APUs (auxiliary power units)..."
Greene: Sixty-five,
FIDO..."
FIDO (Perry): "T-del
confirms throttles." Perry is referring to computer software monitoring
the flight in realtime.
Greene: "...Thank
you."
51.860 - Challenger's main
engines receive commands from the onboard flight computers to begin throttling
back up to 104 percent thrust as planned.
52.000 - Nesbitt: "Velocity
2,257 feet per second (1,539 mph), altitude 4.3 nautical miles, downrange
distance 3 nautical miles..."
57.000 - Scobee, intercom:
"Throttling up."
Smith: "Throttle
up."
Scobee: "Roger."
58.788 - Tracking cameras
show the first evidence of an abnormal plume on the right-hand solid rocket
booster facing away from the shuttle. Scobee and Smith had no data on the
performance of the solid rockets except for a software system that would have
alerted them to malfunctions in the booster steering mechanism.
59.000 - Challenger passes
through the region of maximum aerodynamic pressure, experiencing 720 pounds per
square foot.
59.262 - A continuous
"well defined intense plume" of exhaust is seen on the side of the
suspect booster by tracking cameras. This is clear evidence of a burn through.
59.753 - First visual
evidence of flame on the right-side booster. 70 mm tracking camera closeup: a
flickering tongue of flame appears on side of booster away from shuttle and
quickly becomes continuous.
60.000 - Smith, intercom:
"Feel that mother go!"
Unknown, intercom:
"Wooooo Hooooo!"
60.004 - Data radioed from
Challenger shows the internal pressure in the right-side SRB begins dropping.
This is because of the rapidly increasing hole in the failed joint.
60.238 - First evidence of
flame from the rupture deflecting after impinging on the external fuel tank.
This is a sign that the burn through has increased to the point where the jet
of flame is deflected by the rush of air along the external tank.
60.248 - First evidence of
the anomalous plume "attaching" to the fitting that couples the aft
end of the right-side rocket to the base of the external fuel tank.
60.988 - The plume
deflection is continuous. 70 mm tracking camera closeup: thick, well-defined
plume of flame arcs away from right solid rocket booster.
61.724 - The shuttle rolls
slightly in response to high winds aloft.
62.000 - Smith, intercom:
"Thirty-five thousand, going through one point five."
62.084 - The steering
mechanism of the left-hand booster suddenly moves on computer command as
Challenger's flight control system compensates for wind shear. It is later
noted that wind shear during Challenger's launch was more extreme than for any
of the previous 24 shuttle missions, although still within design limits.
62.484 - Challenger's
computers order the shuttle's right-hand "elevon," or wing flap, to
move suddenly in response to wind.
63.924 - A pressure change
is recorded in the right-hand outboard elevon, indicating movement.
63.964 - The shuttle's
computers order a planned change in Challenger's pitch to ensure the proper
angle of attack during this phase of the trajectory.
64.660 - The plume from the
burn through changes shape suddenly, indicating a leak has started in the
shuttle's liquid hydrogen tank to fuel the fire.
64.705 - A bright,
sustained glow is photographed on the side of the external fuel tank.
64.937 - The main engine
nozzles move through large arcs, trying to keep the shuttle on course as the
flight computers attempt to compensate for the unbalanced thrust produced by
the booster burn through. The shuttle stops the minute pitching. It is doubtful
the crew was aware of the computers' efforts to keep the ship on course. At
this point in the launch phase, the crew is experiencing normal extreme
longitudinal vibrations and steadily increasing acceleration forces. Slight
movement of the shuttle appears visible in NASA's closed-circuit television
system but this could be an illusion.
65.000 - Scobee, intercom:
"Reading four eighty six on mine." This is a routine airspeed
indicator check.
Smith: "Yep, that's
what I've got, too."
65.164 - First recorded
evidence of Challenger experiencing transient motion.
65.524 - Data shows the
left wing's outboard elevon moves suddenly.
66.000 - Booster (Borrer):
"Throttle up, three at 104."
Greene: "Capcom
(Covey), go at throttle up."
66.174 - Tracking cameras
show a bright spot suddenly appears in the exhaust plume from the side of the
right-side solid rocket motor and bright spots are detected on the side of the
rocket facing the belly of the shuttle.
66.764 - The pressure in
the shuttle's external liquid hydrogen tank begins to drop, indicating a
massive leak. Smith had realtime readings of pressure in the liquid hydrogen
tank, but it is doubtful he noticed anything unusual because of the rapidity of
the failure. It made no difference, ultimately, because even if Challenger's pilots had suspected an
SRB problem there was nothing they could have done about it. While the shuttle
separates from its external fuel tank shortly before reaching orbit, it does so
with no engines firing and in a benign aerodynamic environment. As Scobee and
Smith well knew, separating from the tank while the SRBs were firing would
drive the shuttle into the bottom of the fuel tank.
67.650 - The abnormal
plumes on the bottom and top of the booster appear to merge into one. This
means the flame has wrapped around the joint as the leak deteriorated.
67.684 - Telemetry
indicates falling pressure in the 17-inch-wide liquid oxygen propellant lines
feeding the three main engines.
68.000 - Nesbitt:
"Engines are throttling up. Three engines now at 104 percent."
Covey: "Challenger, go
at throttle up."
70.000 - Scobee calmly
responds, air-to-ground: "Roger, go at throttle up."
72.204 - Data shows
divergent up and down motions in nozzles of both solid rocket boosters.
72.284 - The two solid
rocket boosters change position relative to each other, indicating the
right-side booster apparently has pulled away from one of the two struts that
connected its aft end to the external fuel tank. TV tracking camera: A large
ball of orange fire appears higher on other side of main fuel tank, closer to
Challenger's cabin, and grows rapidly.
72.478 - A "major high
rate actuator command" is recorded from one of the boosters, indicating
extreme nozzle motions.
72.497 - The nozzles of the
three liquid-fueled main engines begin moving at high rates: five degrees per
second.
72.525 - Data shows a
sudden lateral acceleration to the right jolts the shuttle with a force of .227
times normal gravity. This is felt by the crew.
72.564 - Start of liquid
hydrogen pressure decrease. Solid rocket boosters again demonstrate high nozzle
motion rates.
72.624 - Challenger beams
back what turns out to be its final navigation update.
72.964 - Main engine liquid
oxygen propellant pressures begin falling sharply at turbopump inlets.
73.000 (approximate) -
Smith, intercom: "Uh oh..." This is the last comment captured by the
crew cabin intercom recorder. Smith may have been responding to indications on
main engine performance or falling pressures in the external fuel tank.
73.010 - Last data is
captured by the tracking and data relay satellite in orbit overhead, indicating
structural breakup has begun in that area.
73.044 - Start of sharp
decrease in liquid hydrogen pressure to the main engines.
73.045 - Another lateral
acceleration, this one to the left, is felt by the crew. Lateral acceleration
equals .254 time the force of gravity.
73.124 - Internal pressure
in the right-side rocket booster is recorded as 19 pounds per square inch below
that of its counterpart, indicating about 100,000 pounds less thrust. Tracking
cameras detect evidence of a circumferential white pattern on the left side of
the base of the external tank indicating a massive rupture near the SRB-tank
attach ring. The is nothing less than the aft dome of the liquid hydrogen tank
blowing out and backwards. The resulting forward acceleration blasts the tank
up into the liquid oxygen tank in the tip of the external fuel tank.
73.137 - Vapors appear near
the intertank section separating the hydrogen and oxygen sections accompanied
by liquid hydrogen spillage from the aft dome of the external tank.
73.143 - All three main
engines respond to loss of oxygen and hydrogen inlet pressure.
73.162 - Ground cameras
show a sudden cloud of rocket fuel appearing along the side of the external
tank. This indicates the nose of the right-hand booster may have pivoted into
the intertank area, compounding the liquid oxygen rupture.
73.191 - A sudden brilliant
flash is photographed between the shuttle and the external tank. TV tracking
camera: Fireballs merge into bright yellow and red mass of flame that engulfs
Challenger. A single crackling noise is heard on air-to-ground radio,
originally thought to be the sound of the explosion transmitted through the
crew's voice-activated microphones. Engineers later determine the sound is the
result of ground transmitters searching the shuttle's frequency range for a
signal.
73.211 - Telemetry data
from the main engines exhibits interference for the next tenth of a second.
73.213 - An explosion
occurs near the forward part of the tank where the solid rocket boosters
attach.
73.282 - The explosion
intensifies and begins consuming the external fuel tank. Television tracking
camera: a ball of brilliant white erupts from the area beneath the shuttle's
nose.
73.327 - The white flash in
the intertank area greatly intensifies.
73.377 - Tank pressure for
on board supplies of maneuvering rocket fuel begins to fluctuate.
73.383 - Data indicates the
liquid-fueled main engines are approaching redline limits on their powerful
fuel pumps.
73.482 - Channel A of main
engine No. 2's control computer votes for engine shutdown because of high
pressure fuel turbopump discharge temperature. Channel B records two strikes
for shutdown.
73.503 - Main engine No. 3
begins shutdown because of high temperatures in its high pressure fuel pump.
Last data captured by main engine No. 3's controller.
73.523 - Main engine No. 1
begins shutdown because of high temperatures in high pressure fuel pump.
73.543 - Last telemetry
from main engine No. 1.
73.618 - The last valid
telemetry from the shuttle is recorded as it breaks up: pressure fluctuations
in a fuel tank in the left rocket pod at Challenger's rear and chamber pressure
changes in auxiliary power unit No. 1's gas generator.
73.631 - End of last data
frame.
74.130 - Last radio signal
from orbiter.
74.587 - A bright flash is
observed in the vicinity of the orbiter's nose. Television tracking camera
closeup: The nose of the shuttle and the crew compartment suddenly engulfed in
brilliant orange flame as rocket fuel in forward maneuvering jet supplies
ignites.
"At that point in its
trajectory, while traveling at a Mach number of 1.92 (twice the speed of sound)
at an altitude of 46,000 feet, the Challenger was totally enveloped in the
explosive burn,"
said the Rogers Commission
report. "The Orbiter, under
severe aerodynamic loads, broke into several large sections which emerged from
the fireball. Separate sections that can be identified on film include the main
engine/tail section with the engines still burning, one wing of the Orbiter,
and the forward fuselage trailing a mass of umbilical lines pulled loose from
the payload bay."
The nose section had ripped
away from the payload bay cleanly, although a mass of electrical cables and
umbilicals were torn from the cargo hold, fluttering behind the crew cabin as
it shot through the thin air, still climbing. Challenger's fuselage was
suddenly open like a tube with its top off. Still flying at twice the speed of
sound, the resulting rush of air that filled the payload bay overpressurized
the structure and it broke apart from the inside out, disintegrating in flight.
Challenger's wings cartwheeled away on their own but the aft engine compartment
held together, falling in one large piece toward the Atlantic Ocean, its engines
on fire because of their sudden shutdown with more oxygen in the system than
hydrogen. The TDRS satellite and its big IUS booster rocket were blown free of
the cargo bay as was Spartan Halley. All this happened as the external tank
gave up its load of fuel, which ignited in the atmosphere in what appeared to
be an explosion. It was more of a sudden burning than an explosion. In any
case, the two solid rockets emerged from the fireball of burning fuel and
continued on, bereft of guidance from the shuttle's now-silent flight
computers.
75.000 - Nesbitt (not
realizing immediately there had been an explosion): "One minute 15
seconds. Velocity 2,900 feet per second (1,977 mph). Altitude 9 nautical miles.
Downrange distance 7 nautical miles."
76.437 - The nose cap of
the right hand solid rocket booster separates and its drogue parachute deploys.
Tracking camera closeup: lone parachute seen emerging from plume of solid
rocket booster.
79.000 - TV tracking
camera, different view: White streamers of smoking debris blossom in all
directions from cloud of smoke and flame marking the spot where Challenger had
been. One large burning piece falls toward the ocean. Two solid rocket boosters
emerge from the fireball and corkscrew through the sky on their own. Nesbitt's
commentary stops.
89.000 - Greene in mission
control utters the first words since the explosion 13 seconds ago: "FIDO,
trajectories..."
FIDO (Perry): "Go
ahead."
Greene: "Trajectory, FIDO."
FIDO: "Flight, FIDO,
filters (radar) got discreting sources. We're go."
Ground control (GC)
engineer N.R. Talbott, mission control: "Flight, GC, we've had negative
contact, loss of downlink (of radio voice or data from Challenger)."
Greene: "OK, all
operators, watch your data carefully."
FIDO: "Flight, FIDO,
till we get stuff back he's on his cue card for abort modes."
Greene: "Procedures,
any help?"
Unknown: "Negative,
flight, no data."
110.250 - Range safety
control officers send radio signals that detonate the self-destruct package on
right-hand solid rocket.
110.252 - The left-hand
booster self destructs. Tracking camera closeup: a thick cloud of black smoke
suddenly engulfs rocket and brilliant but quick explosion ensues. Numerous
fragments of the booster emerge from the fireball, including what appears to be
a complete aft fuel segment, slowly tumbling.
(Editor's Note: The
following times in minutes and seconds)
1:56 - Nesbitt:
"Flight controllers here are looking very carefully at the situation.
Obviously a major malfunction."
2:01 - Ground control
officer: "Flight, GC, negative downlink."
Greene: "Copy."
2:08 - Nesbitt: "We
have no downlink."
2:20 - TV tracking camera:
falling bits of debris create white contrails arching through the blue sky. A
larger object, trailing a thin cloud of vapor, plummets toward the ocean.
2:25 - FIDO: "Flight,
FIDO."
Greene: "Go
ahead."
FIDO: "RSO (range
safety officer) reports vehicle exploded."
Greene (long pause):
"Copy. FIDO, can we get any reports from recovery forces?"
FIDO: "Stand by."
2:45 - Greene: "GC,
all operators, contingency procedures in effect."
2:50 - Nesbitt: "We
have a report from the flight dynamics officer that the vehicle has exploded.
The flight director confirms that. We are looking at checking with the recovery
forces to see what can be done at this point."
3:03 - Greene: "FIDO,
flight..."
FIDO: "Go ahead."
Greene: "LSO (Lockheed
Safety Officer) and recovery forces, any contacts?"
3:09 - Nesbitt:
"Contingency procedures are in effect..."
FIDO: "We're working
with them, flight."
Greene: "OK."
3:22 - Nesbitt: "We
will report more as we have information available. Again, to repeat, we have a
report relayed through the flight dynamics officer that the vehicle has
exploded. We are now looking at all the contingency operations and awaiting
word from any recovery forces in the downrange field."
3:25 - TV tracking camera:
The first pieces of debris can be seen splashing into the ocean.
3:53 - FIDO: "Flight,
FIDO, for what it's worth, the filter shows 'em in the water."
Greene: "Copy."
3:58 - Challenger's crew
cabin smashes into the Atlantic Ocean at about 200 mph. The astronauts, still
strapped in their seats, experience a braking force of 200 times normal
gravity. The crew cabin disintegrates and settles to the bottom 100 feet below.
4:15 - Television tracking
camera closeup shows ocean surface east of Patrick Air Force Station. A large
cloud of ruddy brown smoke hangs over surface of water as objects splash on
impact nearby. The cloud probably was caused by leaking hydrazine rocket fuel
from wreckage that hit the water.
4:27 - Greene: "FIDO,
flight. ... FIDO flight."
FIDO: "Go ahead."
Greene: "Did the RSO's
have an impact point?"
FIDO: "Stand by."
5:03 - Nesbitt: "This
is mission control, Houston. We have no additional word at this time."
5:05 - FIDO: "Flight,
FIDO."
Greene: "Go
ahead."
FIDO: "The vacuum IP
(impact point) is 28.64 North, 80.28 West."
Greene: "How does that
stack with the solid (rocket) recovery forces?" Greene is referring to the
Liberty Star and the Freedom Star, two NASA ships on station in the Atlantic to
recover Challenger's boosters after a normal launch.
FIDO: "We're still
talking to them."
Greene: "OK."
5:24 - Nesbitt:
"Reports from the flight dynamics officer indicate that the vehicle
apparently exploded and that impact in the water (was) at a point approximately
28.64 degrees North, 80.28 degrees West."
5:36 - TV tracking camera:
A dark, irregularly shaped piece of debris - thought to be one of Challenger's
wings- cartwheels down from the sky and splashes into the Atlantic. It is the
largest piece of Challenger seen on TV impacting in the ocean.
5:46 - Nesbitt: "We
are awaiting verification as to the location of the recovery forces in the
field to see what may be possible at this point and we will keep you advised as
further information is available. This is mission control."
6:15 - NASA television
switches from ocean views to the grandstand area at the press site. A large
cloud of white smoke remains visible towering into the sky, twisted by winds
aloft and slowly dissipating. Small, helical streamers mark contrails of the
solid rocket boosters.
6:41 - Greene: "OK,
everybody stay off the telephones, make sure you maintain all your data, start
pulling it together."
7:17 - Greene:
"Flight, FIDO..."
FIDO: "FIDO, flight,
go ahead sir."
Greene: "Are the LSO's
on the loop?"
FIDO: "We can get
'em."
Greene: "Get 'em up on
the loop, please."
LSO: "Yes sir, this is
the LSO."
Greene: "OK, are there
any forces headed out that way?"
LSO: "Yes sir. DOD
(Department of Defense) LSO reports that all ... forces have been scrambled and
they are on their way."
Greene: "OK, do we
have an ETA?"
LSO: "Negative,
sir."
8:00 - Greene conducts a
poll of his flight controllers to determine if any data indicates what may have
gone wrong.
Greene: "Booster,
flight."
Booster: "Flight,
booster."
Greene: "Did you see
anything?"
Booster: "Nothing,
sir, I looked at all the turbine temps were perfect, right on the prediction.
All the redlines were in good shape."
Greene: "RMU?"
RMU (Reiley): "We looked good,
flight."
Greene: "ECOM? ECOM,
flight."
ECOM (Electrical,
environmental and communications systems engineer John Rector): "Flight,
ECOM, we looked normal."
Greene: "DPS?"
DPS (Algate): "All our
data's normal, flight."
Greene: "PROP?"
Propulsion systems (PROP)
engineer A.J. Ceccacci:
"Everything looked good, flight."
Greene: "GNC?"
GNC (Guidance, navigation
and control engineer J.W. Bantle): "Flight, the roll maneuver looked fine,
what we saw of it. We were on our way decreasing roll rate as we lost
data."
Greene: "Copy."
8:03 - NASA select
television shows launch pad 39-B with smoke still hanging over the mobile
launch platform.
8:37 - NASA select
television focuses on a small parachute seen slowly drifting down out to sea.
9:11 - FIDO: "That's,
uh, probably a paramedic." Later it is determined that this is the nose
cap to one of the solid rocket boosters swinging from its drogue parachute.
9:19 - Nesbitt: "This
is mission control, Houston. We are coordinating with recovery forces in the
field. Range safety equipment, recovery vehicles intended for the recovery of
the SRBs in the general area."
9:36 - Greene: "LSO,
flight. LSO, flight..."
Nesbitt: "Those
parachutes believed to be paramedics going into that area..."
FIDO: "We're getting
them, flight."
Nesbitt: "...To
repeat, we had an apparently normal ascent with the data..."
LSO: "This is LSO on
flight loop."
Greene: "Rog, are you
getting any inputs?"
LSO: "Sir, we've got a
Jolly 1 (helicopter) on route right now. We've got ships on the way and we've
got a C-130 on the way out."
Greene: "Rog."
9:41 - Nesbitt:
"...coming from all positions being normal up through approximately time
of main engine throttle back up to 104 percent. At about approximately a minute
or so into the flight, there was an apparent explosion. The flight dynamics
officer reported that tracking reported that the vehicle had exploded and
impact into the water in an area approximately located at 28.64 degrees North,
80.28 degrees West, recovery forces are proceeding to the area including ships
and a C-130 aircraft. Flight controllers reviewing their data here in mission
control. We will provide you with more information as it becomes available.
This is mission control, Houston."
11:05 - NASA select
television shows the interior of mission control at the Johnson Space Center in
Houston. Covey and astronaut Frederick Gregory sit silently at the Capcom
console, obviously stunned.
11:39 - LSO: "Flight,
LSO."
Greene: "Go
ahead."
LSO: "Uh, Jolly's have
not been cleared in yet, there's still debris coming down."
Greene: "Copy. Who's
controlling this operation, please?"
LSO: "S & R
(search and recovery) forces out of Patrick (Air Force Base)."
Greene: "Rog. Do we
have a coordination loop with those people?"
LSO: "We're working
with the SOC on DDMS coord right now." He is referring to a radio network
used by Defense Department personnel.
LSO: "Flight,
LSO."
Greene: LSO..."
LSO: "Would you like
us to try to get up on DDMS coord also?"
Greene: Yes. GC,
flight."
GC: "Flight, GC."
Greene: "Take that
loop into one of the playback loops please, internal to the building
only."
GC: "I didn't copy
what you said."
Greene: "DDMS coord,
patch it into one of the playback loops internal to the building."
GC: "Copy."
12:37 - Greene: "GC,
flight."
GC: "Flight, GC."
Greene: "Checkpoint
status, have we taken one?"
GC: "Negative."
Greene: "Take one
now."
GC: "Copy."
13:27 - GC: "All
flight controllers, hold inputs, lock checkpoint in progress." This is a
procedure to take a "snapshot" of all computer data recorded so far
to ensure its recovery for documentation."
14:24 - Greene: LSO,
flight."
LSO: "LSO here,
sir."
Greene: "Any
updates?"
LSO: "No sir. No sir,
nothing to report."
15:06 - Greene:
"Operators, contingency plan copies are coming to each console position.
If you have an FCOH (flight control operations handbook) you can start on the
checklist, page 27-4, that's page 27-4. Don't reconfigure your console, take
hard copies of all your displays, make sure you protect any data source you
have."
LSO: "Flight,
LSO."
Greene: "LSO?"
LSO: "Looks like about
50 minutes, five zero minutes, before the helicopters are cleared in because of
debris."
Greene: "Fifty minutes
from what time, LSO?"
LSO: "OK, from the
time of the explosion."
21:53 - Nesbitt: "This
is mission control, Houston. Repeating the information that we have at this
time. We had an apparently nominal liftoff this morning at 11:38 Eastern time.
The ascent phase appeared normal through approximately the completion of the
roll program and throttle down and engine throttle back to 104 percent. At that
point, we had an apparent explosion. Subsequent to that, the tracking crews
reported to the flight dynamics officer that the vehicle appeared to have
exploded and that we had an impact in the water down range at a location
approximately 28.64 degrees North, 80.28 degrees west. At the time, the data
was lost with the vehicle. According to a poll by the flight director, Jay
Greene, of the positions here in mission control, there were no anomalous
indications, no indications of problems with engines or with the SRBs or with
any of the other systems at that moment through the point at which we lost
data. Again, this is preliminary information. It is all that we have at the
moment and we will keep you advised as other information becomes available. We
had, there are recovery forces in the general area. Others being deployed,
including aircraft and ships. We saw what we believed to be paramedics
parachuting into impact area and we have no additional word at this point. We
will keep you advised as details become available to us. This is mission
control, Houston."

Challenger's crew departs the Kennedy
Space Center
For additional information about Challenger, see:
http://cbsnews.cbs.com/network/news/space/51Lintro.html
STS-107
 The
shuttle Columbia blasted off on mission STS-107 at 10:39 a.m. on Jan. 16, 2003.
At the controls were commander Rick Husband, pilot William "Willie"
McCool, flight engineer Kalpana Chawla, physician Laurel Clark, payload
commander Michael Anderson, physician David Brown and Israeli astronaut Ilan
Ramon. STS-107 was one of only two flights left on the shuttle manifest that
were not bound for the international space station (the other was a Hubble
Space Telescope servicing mission).
The
shuttle Columbia blasted off on mission STS-107 at 10:39 a.m. on Jan. 16, 2003.
At the controls were commander Rick Husband, pilot William "Willie"
McCool, flight engineer Kalpana Chawla, physician Laurel Clark, payload
commander Michael Anderson, physician David Brown and Israeli astronaut Ilan
Ramon. STS-107 was one of only two flights left on the shuttle manifest that
were not bound for the international space station (the other was a Hubble
Space Telescope servicing mission).
The goal of the 16-day mission was to carry out space station-class research in a variety of disciplines, ranging from biology to medicine, from materials science to pure physics and technology development, research that, for a variety of reasons, had never made it to the international space station.
Columbia's launching appeared normal, but analysis of tracking camera footage later that day showed a large chunk of foam insulation broke away from the shuttle's external tank about 81 seconds after liftoff. The foam appeared to come from a the left bipod ramp, an aerodynamically shaped ramp of foam built up around one of the two struts holding the nose of the shuttle to the tank. The foam fell along the tank and disappeared under Columbia's left wing. A shower of whitish debris was seen an instant later exiting from under the wing. The foam had obviously struck the wing, but where? And what sort of damage, if any, did it cause?
Engineers ultimately would conclude the impact likely caused no entry-critical damage. Husband and his crew were only informed about the strike in passing, in an email from mission managers who were concerned the astronauts might hear about the strike from reporters during upcoming on-orbit interviews. As it turned out, only a few reporters even knew about the foam strike and no one asked the crew about it. For their part, Husband and company chalked up a near perfect science mission before packing up for the trip back to Earth.
The day before re-entry, flight director LeRoy Cain downplayed the foam strike, saying engineers "took a very thorough look at the situation with the tile on the left wing and we have no concerns whatsoever. We haven't changed anything with respect to our trajectory design. It will be a nominal, standard trajectory."
He was wrong.
Shuttle Columbia destroyed in
entry mishap
By WILLIAM HARWOOD
CBS News
The shuttle Columbia suffered a catastrophic failure returning to Earth Saturday, breaking apart 207,135 feet above Texas en route to a landing at the Kennedy Space Center to close out a 16-day science mission. The shuttle's seven-member crew - two women and five men, including the first Israeli space flier - perished in the disaster, the first loss of life on the high frontier since the 1986 Challenger disaster.
The initial phases of the descent went normally and Columbia crossed above the coast of California just north of San Francisco around 5:51 a.m. local time, or 8:51 a.m. EST, on track for a landing on runway 33 at the Kennedy Space Center just 25 minutes later at 9:16 a.m.
The first sign of anything unusual came at 8:53 a.m., when the shuttle was flying high above the heartland of America.
Telemetry showed a sudden loss of hydraulic system data from the inboard and outboard wing flaps, or elevons, on Columbia's left wing. Three minutes later, sensors in the brake lines and tires of the shuttle's left-side main landing gear suddenly stopped providing data.
The shuttle continued to fly in a normal manner with no hint that a catastrophic failure was imminent.
Then at 8:58 a.m., sensors that monitor temperatures where the shuttle's protective thermal tiles are glued or bonded to the airframe suddenly dropped out followed one minute later by loss of data from landing gear pressure sensors on the left side tires. Columbia's flight computers alerted the astronauts to the pressure indication and one of the crew members acknowledged the alert in a brief call to mission control.
That was the final transmission from the space shuttle. Moments later, all data were lost and the vehicle broke up while traveling 18.3 times the speed of sound. Mission duration to that point was 15 days 22 hours 20 minutes and 22 seconds, translating to 8:59:22 a.m. EST (Editor's note: This time was later amended; see the detailed timeline below for exact timing). Wreckage was soon found strewn over a debris "footprint" stretching across eastern Texas and into Louisiana. There was no immediate word on where Columbia's reinforced crew module might have crashed to Earth.

In a brief address to the nation, President Bush said "this day has brought terrible news and great sadness to our country. ... Columbia is lost. There are no survivors."
"The same creator who names the stars also knows the names of the seven souls we mourn today," he said. "The crew of the shuttle Columbia did not return safely to Earth. Yet we can pray they are all safely home."
Said NASA Administrator Sean O'Keefe: "The loss of this valiant crew is something we will never be able to get over."
Family members were standing by at the shuttle runway to welcome their loved ones back to Earth. William Readdy, NASA's associate administrator for space flight and a veteran shuttle commander, praised the astronauts' families for showing an "incredible amount of dignity considering their loss."
"They knew the crew was absolutely dedicated to the mission they were performing," he said, barely able to control his emotions. "They believed in what they were doing and in the conversations with the families, they said we must find what happened, fix it and move on. We can't let their sacrifice be in vain.
"Today was a very stark reminder this is a very risky endevour, pushing back the frontiers in outer space. Unfortunately, people have a tendency to look at it as something that is more or less routine. I can assure you, it is not.
"I have to say as the one responsible for shuttle and (space) station within NASA, I know the people in NASA did everything possible preparing for this flight to make it as perfect as possible," Readdy said. "My promise to the crew and the crew families is the investigation we just launched will find the cause. We'll fix it. And then we'll move on."
The goal of mission STS-107 was to carry out space station-class research in a variety of disciplines, ranging from biology to medicine, from materials science to pure physics and technology development, research that cannot yet be accommodated on the still-unfinished international space station.
More than 80 experiments were on board, most of them in a Spacehab research module in Columbia's cargo bay. To collect as much data as possible, the astronauts worked around the clock in two 12-hour shifts. By all accounts, the crew accomplished all of their major objectives.
At an afternoon news conference, shuttle program Ronald Dittemore and senior flight director Milt Heflin reviewed the telemetry from the shuttle and answered as many questions as possible. NASA's openness during the immediate aftermath of a devastating day was in stark contrast to the strict "no comment" policy implemented in the wake of the 1986 Challenger disaster that frustrated the public and tarnished the agency's reputation for openness.
"We're devastated because of the events that unfolded this morning," Dittemore said. "There's a certain amount of shock in our system because we have suffered the loss of seven family members. And we're learning to deal with that. Certainly, a somber mood in our teams as we continue to try to understand the events that occurred, but our thoughts and our prayers go out to the families.
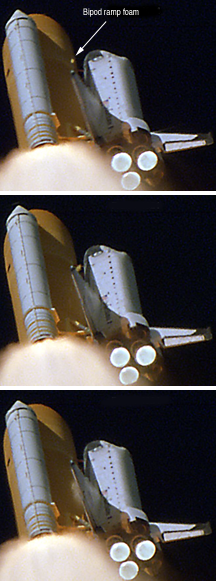
"As difficult as this is for us, we wanted to meet with you and be as fair and open with you (as possible), given the facts as we understand them today," he said. "We will certainly be learning more as we go through the coming hours, days and weeks. We'll tell you as much as we know, we'll be as honest as we can with you and certainly we'll try to fill in the blanks over the coming days and weeks."
10:40:22 a.m., Jan. 16, 2003: A briefcase-size chunk of foam
breaks away from the left bi-pod ramp of Columbia's external fuel tank 81.7
seconds after liftoff as seen in these enhanced video frames from a NASA
tracking camera. The shuttle's velocity is 1,568 mph and the foam breaks into
several pieces as it tumbles in the airstream. In two-tenths of a second, the
largest piece of debris slows to 1,022 mph as it disappears behind Columbia's
left wing (photo 3). It emerges in a powdery looking shower of debris after
hitting the wing at a relative velocity of about 545 mph.
An internal NASA team of senior managers was named to handle the initial investigation into the disaster. An independent team of experts also was named to ensure objectivity. All flight control data and shuttle telemetry was impounded and "tiger teams" were formed to begin the painful tasks of sifting the data and coordinating the recovery of debris.
Dittemore said the shuttle fleet will remain grounded until engineers pinpoint what went wrong with Columbia and determine what corrections might be necessary.
Columbia's flight was one of only two remaining on NASA's long term launch schedule that does not involve the international space station. NASA had planned to launch the shuttle Atlantis around March 6 to ferry a fresh crew to the station and to bring the lab's current occupants back to Earth after 114 days in space.
Around 9:30 a.m. Saturday, flight controllers informed Expedition 6 commander Kenneth Bowersox, flight engineer Nikolai Budarin and science officer Donald Pettit that Columbia had been lost during re-entry.
Bowersox and his crewmates have enough on-board supplies to remain aloft aboard the station through June. In fact, an unmanned Russian Progress supply ship is scheduled for launch Sunday from the Baikonur Cosmodrome in Kazakstan. That launch will proceed as planned, officials said.
If the shuttle fleet remains grounded through June, the station crew could be forced to abandon the station and return to Earth aboard a Russian Soyuz lifeboat. Fresh lifeboats are delivered to the station every six months to ensure the crew has a way to bail out in case of problems with the shuttle fleet or some other in-flight emergency.
With enough supplies on board to last Bowersox and his crewmates until late June, "there's some time for us to work through this," Dittemore said. "Right now, certainly there is a hold on future flights until we get ourselves established and understand the root cause of this disaster."
Dittemore provided a sense of the loss felt by NASA and its contractors when he said "it's an emotional event, when we work together, we work together as family member and we treat each other that way. ... It's a sad loss for us.
"We understand the risks that are involved in human spaceflight and we know these risks are manageable and we also know they're serious and can have deadly consequences," he said. "So we are bound together with the threat of disaster all the time. ... We all rely on each other to make each spaceflight successful. So when we have an event like today, when we lose seven family members, it's just devastating to us."
Columbia blasted off on the 113th shuttle mission Jan. 16. The climb to space appeared uneventful, but about one minute and 20 seconds after liftoff, long-range tracking cameras showed a piece of foam insulation from the shuttle's external tank breaking away and hitting Columbia's left wing. The foam came from near the area where a forward bipod assembly attaches the nose of the shuttle to the tank. The debris hit the left wing near its leading edge.
Entry flight director Leroy Cain said Friday a detailed analysis of the debris impact led engineers to believe there was no serious damage. Columbia was not equipped with a robot arm for this Spacehab research mission and the impact area was not visible from the shuttle's crew cabin.
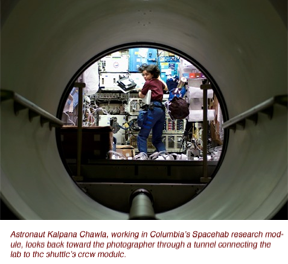
Whether the debris caused enough damage to compromise the integrity of the wing's thermal protection system is not yet known. But when the failure occurred, the shuttle was experiencing maximum heat loads of nearly 3,000 degrees Fahrenheit.
"If we did have a structural problem or a thermal problem, you would expect to get it at the peak heating," he said. "The most extreme thermal environment was right at mach 18 and that's where we lost the vehicle."
The shuttle Challenger was destroyed in 1986 by the failure of an O-ring seal in one of the ship's two solid-fuel boosters. All seven crew members perished, including New Hampshire social studies teacher Christa McAuliffe. McAuliffe's backup, Idaho teacher Barbara Morgan, witnessed the disaster from the NASA press site 4.2 miles from Challenger's launch pad.
In a painful footnote to Saturday tragedy, Morgan was once again at the Kennedy Space Center, this time as a full-time astronaut awaiting launch in November on Columbia's next mission. Morgan is the first member of a new class of educator astronauts, part of a program initiated by O'Keefe to help generate more student interest in science and technology.
Since the educator-astronaut program was announced last month, more than 1,000 teachers have expressed interest or been nominated as potential candidates by students, family members or friends. The status of that program, and the impact of Columbia's loss on Morgan's flight, is not yet known.
But as President Bush promised family members and the nation Saturday, "the cause for which they died will continue. ... Our journey into space will go on."
o o
o
In the days, weeks and months ahead, an investigation of the disaster revealed echoes of Challenger: a long history of foam insulation problems that represented an unrecognized risk; bureaucratic inertia; slipshod internal communications and ineffective management at the top levels of NASA. The Columbia Accident Investigation Board, lead by retired Navy Adm. Harold Gehman, issued its report Aug. 28, 2005, concluding the so-called "NASA culture" was deeply flawed and in need of major modifications to prevent a repeat of the Columbia disaster in the years ahead.
"Based on NASA's history of ignoring external recommendations, or making improvements that atrophy with time, the Board has no confidence that the space shuttle can be safely operated for more than a few years based solely on renewed post-accident vigilance," the report stated.
Continuing, the report said that unless NASA took strong action to change its management culture to enhance safety margins in shuttle operations, "we have no confidence that other 'corrective actions' will improve the safety of shuttle operations. The changes we recommend will be difficult to accomplish - and they will be internally resisted."
For an agency with such a proud tradition - sending 12 men to the surface of the moon, establishing a permanent presence in low Earth orbit, exploring the solar system with unmanned robots and launching scientific sentinels to probe the depths of space and time - the criticism levied by the accident board seemed extreme in its harshness.
But the accident investigation board members and their investigators clearly believed the sharp tone was appropriate, in their view essential to ensuring that wide-ranging corrective actions would be actually implemented. The board's investigation found that "management decisions made during Columbia's final flight reflect missed opportunities, blocked or ineffective communications channels, flawed analysis and ineffective leadership."

Photographer Gene Blevins captured this
shot of Columbia streaking
high above California minutes before
its destruction. By this point,
Columbia's left wing was in the process
of melting from the inside out.
In the end, the report concluded, NASA managers never really understood the lessons of the 1986 Challenger disaster and "echoes of Challenger" abounded in the miscues that led to Columbia's destruction.
"Connecting the parts of NASA's organizational system and drawing the parallels with Challenger demonstrate three things," the board found. "First, despite all the post-Challenger changes at NASA and the agency's notable achievements since, the causes of the institutional failure responsible for Challenger have not been fixed.
"Second, the Board strongly believes that if these persistent, systemic flaws are not resolved, the scene is set for another accident. Therefore, the recommendations for change are not only for fixing the shuttle's technical system, but also for fixing each part of the organizational system that produced Columbia's failure.
"Third, the Board's focus on the context in which decision making occurred does not mean that individuals are not responsible and accountable. To the contrary, individuals always must assume responsibility for their actions. What it does mean is that NASA's problems cannot be solved simply by retirements, resignations, or transferring personnel."
The 13-member Columbia Accident Investigation Board spent seven months investigating the Feb. 1 Columbia disaster, reviewing more than 30,000 documents, conducting more than 200 formal interviews and collecting testimony from expert witnesses. The board also oversaw debris recovery efforts in Texas and Louisiana that involved more than 25,000 searchers. The investigation was expected to cost $19.8 million when all was said and done.
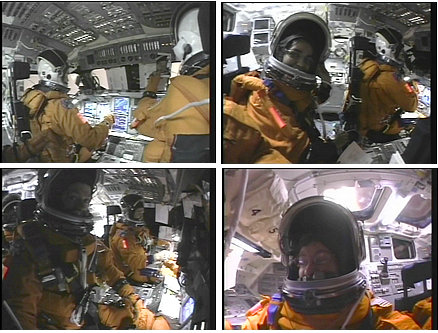 "
"
Columbia's flight deck, as captured by a videocamera operated
by Laurel Clark, 15 minutes before the shuttle's destruction Feb. 1, 2003. In
the top left frame, the heat of re-entry is evident out the windows in front of
commander Rick Husband and pilot Willie McCool. In the top right frame, Chawla
smiles for the camera. Bottom right: Clark turns the camera on herself.
The board's 248-page report was released at the National Transportation and Safety Board in Washington. Reporters were allowed to review the report ahead of time, surrendering cell phones and wireless laptop network cards before entering a closed off "reading room" at 6 a.m. Gehman and other members of the panel discussed the report during a news conference.
"The people of NASA have accomplished great things," Dana Rohrabacher, D-Calif., chairman of a key House space committee, told CBS News. "They've put a man on the moon within a very short period of time, the people of NASA have been a source of great pride ... for the people of the United States.
"But for far too long, they've been resting on their laurels and bathing in past glories, nostalgic about the glory days," he continued. "It's time to look to the future and it's time to recapture a tough, hard-working body of people who have new challenges and are not just looking at the past but looking to the future. And that means Congress and the president have got to act on the Gehman report."
 The
CAIB report focused on two broad themes: The direct cause of the disaster -
falling external fuel tank foam insulation that blasted a deadly hole in the
leading edge of Columbia's left wing 82 seconds after liftoff - and the
management system that failed to recognize frequent foam shedding as a
potentially lethal defect before Columbia even took off.
The
CAIB report focused on two broad themes: The direct cause of the disaster -
falling external fuel tank foam insulation that blasted a deadly hole in the
leading edge of Columbia's left wing 82 seconds after liftoff - and the
management system that failed to recognize frequent foam shedding as a
potentially lethal defect before Columbia even took off.
The report also focuses on how NASA's mission management team, a panel of senior agency managers responsible for the day-to-day conduct of Columbia's mission, failed to recognize the severity of the foam strike that actually occurred, virtually eliminating any chance to save the shuttle's crew, either by attempting repairs in orbit or launching a rescue mission.
The report made 29 recommendations, 15 of which were to be implemented before shuttle flights resumed. Five of those were released earlier, requiring NASA to eliminate foam shedding to the maximum extent possible; to obtain better imagery from the ground and in orbit to identify any problems with the shuttle's thermal protection system; and development of tools and procedures to repair any such damage in space.
The more difficult recommendations addressed management changes and the establishment of an independent Technical Engineering Authority to verify launch readiness, oversee and coordinate requests
for waivers and to "decide what is and is not an anomalous event." The TEA "should have no connection to or responsibility for schedule and program cost." In addition, the report concluded, NASA's Office of Safety and Mission Assurance should have direct authority over all shuttle safety programs and be independently funded.
"It is the Board's opinion that good leadership can direct a culture to adapt to new realities," the panel wrote. "NASA's culture must change, and the Board intends (its) recommendations to be steps toward effecting this change."
The foam strike that doomed Columbia was not seen until the day after launch when engineers began reviewing tracking camera footage as they do after every launching. A film camera in Cocoa Beach that could have photographed the impact on the underside of the left wing was out of focus. A video camera at the same site was properly focused, but it lacked the resolution, or clarity, to show exactly where the foam hit or whether it caused any damage. A third camera at a different site showed the foam disappearing under the left wing and emerging as a cloud of debris after striking the underside. Again, the exact impact point could not be seen.
Stunned engineers immediately began analyzing the available film and video and ultimately determined the foam had struck heat shield tiles on the underside of the wing, perhaps near the left main landing gear door. No one ever seriously considered a direct heat on the reinforced carbon carbon panels making up the wing leading edge because no trace of foam debris was ever seen crossing the top of the wing. As the board ultimately concluded, however, the foam did, in fact, strike the leading edge on the lower side of RCC panel No. 8.
In hindsight, it's difficult to understand why the possibility of a leading edge impact didn't receive more attention. The board concluded that was due at least in part to the influential role of Calvin Schomburg, a senior engineer at the Johnson Space Center with expertise in the shuttle's heat-shield tiles.
"Shuttle program managers regarded Schomburg as an expert on the thermal protection system," the board wrote. "However, the board notes that Schomburg as not an expert on reinforced carbon carbon (RCC), which initial debris analysis indicated the foam may have struck. Because neither Schomburg nor shuttle management rigorously differentiated between tiles and RCC panels, the bounds of Schomburg's expertise were never properly qualified or questioned."
 In
any case, a team of Boeing engineers at the Johnson Space Center, under
direction of NASA's mission management team, ultimately concluded the foam
strike did not pose a safety of flight issue. Their analysis, using a computer
program called CRATER, predicted areas of localized, possibly severe damage to
the underside of the left wing, but no catastrophic breach. The concern,
rather, was that any damage likely would require extensive repairs before
Columbia could fly again.
In
any case, a team of Boeing engineers at the Johnson Space Center, under
direction of NASA's mission management team, ultimately concluded the foam
strike did not pose a safety of flight issue. Their analysis, using a computer
program called CRATER, predicted areas of localized, possibly severe damage to
the underside of the left wing, but no catastrophic breach. The concern,
rather, was that any damage likely would require extensive repairs before
Columbia could fly again.
While the damage assessment was getting under way, at least three different attempts were made to obtain spy satellite photography of the impact site to resolve the matter one way or the other. But in a series of communications miscues, the efforts ultimately were quashed by the MMT, under the direction of former flight director Linda Ham.
Ham said she was never able to find out who wanted such photographs and, without a formal requirement, had no reason to proceed. As for the debris assessment, Ham and other members of the MMT never challenged the hurried analysis or questioned the conclusion Columbia could safely return to Earth as is.
Many mid-level engineers said later they had serious misgivings about the debris assessment and heavy email traffic indicated fairly widespread concern about potentially serious problems if the foam strike had compromised Columbia's left main landing gear. Yet those concerns never percolated up the Ham, Dittemore or other members of the mission management team.
Ham and Dittemore both have said they were always open for questions or comments from lower-level engineers and that everyone on the team was encouraged, even duty bound, to bring any serious concerns to the attention of senior management.
But the CAIB disagreed.
"Communication did not flow effectively up to or down from program managers," the board wrote. "After the accident, program managers stated privately and publicly that if engineers had a safety concern, they were obligated to communicate their concerns to management. Managers did not seem to understand that as leaders they had a corresponding and perhaps greater obligation to create viable routes for the engineering community to express their views and receive information. This barrier to communications not only blocked the flow of information to managers but it also prevented the downstream flow of information from managers to engineers, leaving Debris Assessment Team members no basis for understanding the reasoning behind Mission Management Team decisions."
As for not hearing any dissent, the board wrote, "managers' claims that they didn't hear the engineers' concerns were due in part to their not asking or listening."
"Management decisions made during Columbia's final flight reflect missed opportunities, blocked or ineffective communications channels, flawed analysis and ineffective leadership," the board wrote. "Perhaps most striking is the fact that management - including Shuttle Program, Mission Management Team, Mission Evaluation Room (personnel) and flight director and mission control - displayed no interest in understanding a problem and its implications.
"Because managers failed to avail themselves of the wide range of expertise and opinion necessary to achieve the best answer to the debris strike question - 'Was this a safety-of-flight concern?' - some space shuttle program managers failed to fulfill the implicit contract to do whatever is possible to ensure the safety of the crew. In fact, their management techniques unknowingly imposed barriers that kept at bay both engineering concerns and dissenting views and ultimately helped create 'blind spots' that prevented them from seeing the danger the foam strike posed."
Shuttle program manager Dittemore and members of the mission management team "had, over the course of the space shuttle program, gradually become inured to external tank foam losses and on a fundamental level did not believe foam striking the vehicle posed a critical threat to the orbiter," the board wrote.
 In
the end, it was a moot point. Once the foam breached the leading edge of
Columbia's left wing, the crew was doomed. The astronauts had no way to repair
the breach - no robot arm and no tile repair equipment - and there was no
realistic chance another shuttle could be readied in time for a rescue mission.
In
the end, it was a moot point. Once the foam breached the leading edge of
Columbia's left wing, the crew was doomed. The astronauts had no way to repair
the breach - no robot arm and no tile repair equipment - and there was no
realistic chance another shuttle could be readied in time for a rescue mission.
Maybe so. But NASA's flawed management system never gave the agency a chance to prove it still had the "right stuff." And it was that institutional system, or "culture," at NASA that must be changed, the board said, to prevent another accident.
"An organization system failure calls for corrective measures that address all relevant levels of the organization, but the Board's investigation shows that for all its cutting-edge technologies, 'diving-catch' rescues and imaginative plans for the technology and the future of space exploration, NASA has shown very little understanding of the inner workings of its own organization," the report states.
"NASA's bureaucratic structure kept important information from reaching engineers and managers alike. The same NASA whose engineers showed initiative and a solid working knowledge of how to get things done fast had a managerial culture with an allegiance to bureaucracy and cost-efficiency that squelched the engineers' efforts.
"When it came to managers' own actions, however, a different set of rules prevailed. The Board found that Mission Management Team decision-making operated outside the rules even as it held its engineers to a stifling protocol. Management was not able to recognize that in unprecedented conditions, when lives are on the line, flexibility and democratic process should take priority over bureaucratic response."
NASA Administrator Sean O'Keefe said the space agency would use the Columbia Accident Investigation Board's final report as a blueprint for correcting the problems that led to Columbia's demise.
"We have accepted the findings and will comply with the recommendations to the best of our ability," O'Keefe said in a statement. "The board has provided NASA with an important road map as we determine when we will be 'fit to fly' again.
"Due to the comprehensive, timely and open public communication displayed by the Board throughout the investigative process, we already have begun to take action on the earlier issued recommendations, and we intend to comply with the full range of recommendations released today."
Gehman told CBS News after the CAIB report was released that NASA had little choice. In the panel's view, he said, NASA could not safely operate the space shuttle program without major changes in its management system.
"I think there's a little bit of denial that NASA, at least in the shuttle program, that NASA has modified its organizational structure over the years into one that no longer contains the attributes that they built their reputations on," Gehman said. "There may be some people who deny that, but the board is absolutely convinced, we think there's no room for any doubt whatsoever, the management system they have right now is not capable of safely operating the shuttle over the long term. That's the bottom line."
Gehman also said Congress and the White House must share blame for the Columbia disaster with NASA. Asked what he might tell President Bush about NASA and the agency's second in-flight tragedy, Gehman said he would point out that "NASA is a great organization that he and the country can have a lot of pride in. And that they are operating under and unrealistic set of rules and guidelines."
 "Exploring
space on a fixed cost basis is not realistic," the retired admiral said.
"Launching shuttles on a calendar basis instead of an event-driven basis
is not realistic. Demanding that you save money and run this thing in an
efficient and effective way and that you get graded on schedule and things like
that is not realistic. That the whole nation and Congress and the White House
has an unrealistic view of how we do space exploration."
"Exploring
space on a fixed cost basis is not realistic," the retired admiral said.
"Launching shuttles on a calendar basis instead of an event-driven basis
is not realistic. Demanding that you save money and run this thing in an
efficient and effective way and that you get graded on schedule and things like
that is not realistic. That the whole nation and Congress and the White House
has an unrealistic view of how we do space exploration."
In addition, the board's report "clearly specifies that there is responsibility at both ends of Pennsylvania Avenue for this that are shared with NASA," Gehman said. "Now in some cases, NASA over markets what they can do. They promise more than they can deliver and they promise they can deliver it at a price that is less than it's really going to cost. But in some cases, it is demanded of them, in order to get a program approved, that they agree to unrealistic schedules and unrealistic price tags. So there's blame at both ends here."
The CAIB report focused heavily on decisions made by NASA's mission management team. But Gehman told CBS News the space agency's management system was so dysfunctional it hardly mattered who was in charge.
"We believe very, very strongly that you could substitute almost anybody in those positions and operate under the guidelines and rules and precedents that were being used in NASA and they would make the same errors," he said.
"Let me give you a specific case in point. Much has been made of the fact that the MMT didn't meet every day. NASA regulations require that they meet every day. So I had my board go back and see what were the meetings scheduled for the previous two shuttle missions? Guess what? They met every third day.
"So Linda Ham was doing her job according to the standards and precedents that were set by the establishment," he continued. "Even though the rules say you have to meet every day, you don't really have to. So that's an organizational flaw and she was performing her duties in that respect in accordance with the standards and precedents that had been previously established by her predecessors. And her predecessor's bosses had let that go on.
"So we feel very, very strongly that just moving the people around won't fix that problem. Unfortunately, we live in a town here in Washington, DC, in which they frequently demand someone pay. But we on the board were not influenced by that" and the board did not assign personal blame for any real or perceived errors in judgment.
Could a more experienced or proactive program manager or MMT chairman have made a different in Columbia's case?
"We feel there's some part of this, maybe even a lot of these problems, could have been mitigated by a stronger, a more suspicious, nervous kind of a person," Gehman said of the MMT and its chairman. "But our conclusion, our very, very strong conclusion is even if you had really brilliant people, really spectacular people, if you had the very, very best person you could get, that it would be a low probability bet that you could count on them to overcome the flaws in the organization. That is a low probability course of action."
Asked if NASA was "in denial" about serious management flaws and defects, Gehman said "in a lot of cases, they will deny that they have a basic organizational flaw which is dangerous. I think they'll deny that, some of them. Others will applaud it. It kind of depends on where you sit."
The CAIB's criticism of NASA drew an unusual response from Stephen Feldman, president of The Astronauts Memorial Foundation.
"One of the great risks of the Columbia tragedy and the subsequent report and commentary is that outstanding scientists and engineers may feel so criticized and unappreciated that they will leave NASA and the space program for higher paying and often less stressful jobs in the private sector," he said in a statement. "The outstanding safety record that NASA has compiled over the years shouldn't be forgotten because of one terrible accident on February 1, 2003."
But O'Keefe's promise to full implement the CAIB recommendations drew praise from the National Space Society, a nonprofit advocacy group founded by German rocket scientist Wernher von Braun.
"The National Space Society urges NASA to embrace the recommendations of the CAIB and work diligently to fundamentally reform its decision-making processes and safety organizations so that we can safely return the Space Shuttle fleet to service," said Executive Director Brian Chase. "However, in order for NASA to fully implement the CAIB recommendations and continue the exploration of space, the agency will need appropriate funding to accomplish those tasks.
"The White House and the U.S. Congress must accept their share of responsibility for the future of our nation's space exploration efforts and provide the necessary leadership.
"Perhaps most importantly, NASA and our nation's leaders need to take this opportunity to foster development of new space transportation systems and renew a long-term commitment to human space exploration."
Four and a half months after the CAIB report was released, President Bush gave a speech at NASA Headquarters in Washington in which he called for retirement of the shuttle by 2010; development of a new manned "crew exploration vehicle; the establishment of a permanent base on the moon by 2020 and eventual manned flights to Mars.
o o
o
Recommendations of the Columbia Accident Investigation
Board
PART ONE
– THE ACCIDENT
Thermal Protection System
1 Initiate
an aggressive program to eliminate all External Tank Thermal Protection System debris-shedding
at the source with particular emphasis on the region where the bipod struts
attach to the External Tank. [RTF]
2 Initiate
a program designed to increase the Orbiter's ability to sustain minor debris
damage by measures such as improved impact-resistant Reinforced Carbon-Carbon
and acreage tiles. This program should determine the actual impact resistance
of current materials and the effect of likely debris strikes. [RTF]
3 Develop
and implement a comprehensive inspection plan to determine the structural
integrity of all Reinforced Carbon-Carbon system components. This inspection
plan should take advantage of advanced non-destructive inspection technology.
[RTF]
4 For
missions to the International Space Station, develop a practicable capability
to inspect and effect emergency repairs to the widest possible range of damage
to the Thermal Protection System, including both tile and Reinforced
Carbon-Carbon, taking advantage of the additional capabilities available when
near to or docked at the International Space Station.
For non-Station missions, develop a comprehensive
autonomous (independent of Station) inspection and repair capability to cover
the widest possible range of damage scenarios.
Accomplish an on-orbit Thermal Protection System
inspection, using appropriate assets and capabilities, early in all missions.
The
ultimate objective should be a fully autonomous capability for all missions to
address the possibility that an International Space Station mission fails to
achieve the correct orbit, fails to dock successfully, or is damaged during or
after undocking. [RTF]
5 To
the extent possible, increase the Orbiter's ability to successfully re-enter
Earth's atmosphere with minor leading edge structural sub-system damage.
6 In
order to understand the true material characteristics of Reinforced
Carbon-Carbon components, develop a comprehensive database of flown Rein-forced
Carbon-Carbon material characteristics by destructive testing and evaluation.
7 Improve
the maintenance of launch pad structures to minimize the leaching of zinc
primer onto Reinforced Carbon-Carbon components.
8 Obtain
sufficient spare Reinforced Carbon-Car-bon panel assemblies and associated support
components to ensure that decisions on Rein-forced Carbon-Carbon maintenance
are made on the basis of component specifications, free of external pressures
relating to schedules, costs, or other considerations.
9 Develop,
validate, and maintain physics-based computer models to evaluate Thermal
Protection System damage from debris impacts. These tools should provide
realistic and timely estimates of any impact damage from possible debris from
any source that may ultimately impact the Orbiter. Establish impact damage
thresholds that trigger responsive corrective action, such as on-orbit
inspection and repair, when indicated.
Imaging
10 Upgrade
the imaging system to be capable of providing a minimum of three useful views
of the Space Shuttle from liftoff to at least Solid Rocket Booster separation,
along any expected ascent azimuth. The operational status of these assets
should be included in the Launch Commit Criteria for future launches. Consider
using ships or aircraft to provide additional views of the Shuttle during
ascent. [RTF]
11 Provide
a capability to obtain and downlink high-resolution images of the External Tank
after it separates. [RTF]
12 Provide
a capability to obtain and downlink high-resolution images of the underside of
the Orbiter wing leading edge and forward section of both wings' Thermal
Protection System. [RTF]
13 Modify
the Memorandum of Agreement with the National Imagery and Mapping Agency to
make the imaging of each Shuttle flight while on orbit a standard requirement.
[RTF]
Orbiter Sensor Data
14 The
Modular Auxiliary Data System instrumentation and sensor suite on each Orbiter
should be maintained and updated to include current sensor and data acquisition
technologies.
15 The
Modular Auxiliary Data System should be redesigned to include engineering
performance and vehicle health information, and have the ability to be
reconfigured during flight in order to allow certain data to be recorded,
telemetered, or both as needs change.
Wiring
16 As
part of the Shuttle Service Life Extension Program and potential 40-year
service life, develop a state-of-the-art means to inspect all Orbiter wiring,
including that which is inaccessible
Bolt Catchers
17 Test
and qualify the flight hardware bolt catchers. [RTF]
Closeouts
18 Require
that at least two employees attend all final closeouts and intertank area
hand-spraying procedures. [RTF]
Micrometeoroid and Orbital Debris
19 Require
the Space Shuttle to be operated with the same degree of safety for
micrometeoroid and orbital debris as the degree of safety calculated for the
International Space Station. Change the micrometeoroid and orbital debris
safety criteria from guidelines to requirements.
Foreign Object Debris
20 Kennedy
Space Center Quality Assurance and United Space Alliance must return to the
straightforward, industry-standard definition of “Foreign Object Debris” and
eliminate any al-ternate or statistically deceptive definitions like
“processing debris.” [RTF]
PART TWO
– WHY THE ACCIDENT OCCURRED
Scheduling
21 Adopt
and maintain a Shuttle flight schedule that is consistent with available
resources. Although schedule deadlines are an important management tool, those
deadlines must be regularly evaluated to ensure that any additional risk
incurred to meet the schedule is recognized, understood, and acceptable. [RTF]
Training
22 Implement
an expanded training program in which the Mission Management Team faces
potential crew and vehicle safety contingencies beyond launch and ascent. These
contingencies should involve potential loss of Shuttle or crew, contain
numerous uncertainties and unknowns, and require the Mission Management Team to
assemble and interact with support organizations across NASA/Contractor lines and
in various locations. [RTF]
Organization
23 Establish
an independent Technical Engineering Authority that is responsible for
technical requirements and all waivers to them, and will build a disciplined,
systematic approach to identifying, analyzing, and controlling hazards
throughout the life cycle of the Shuttle System. The independent technical
authority does the following as a minimum:
• Develop and maintain
technical standards for all Space Shuttle Program projects and elements
• Be the sole waiver-granting
authority for all technical standards
• Conduct trend and risk
analysis at the sub-system, system, and enterprise levels
• Own the failure mode,
effects analysis and hazard reporting systems
• Conduct integrated hazard
analysis
• Decide what is and is not
an anomalous event
• Independently verify
launch readiness
• Approve the provisions of
the recertification program called for in Recommendation R9.1-1. The Technical
Engineering Authority should be funded directly from NASA Headquarters, and
should have no connection to or responsibility for schedule or program cost.
24 NASA
Headquarters Office of Safety and Mission Assurance should have direct line
authority over the entire Space Shuttle Program safety organization and should
be independently re-sourced.
25 Reorganize
the Space Shuttle Integration Office to make it capable of integrating all
elements of the Space Shuttle Program, including the Or-biter.
PART THREE – A LOOK AHEAD
Organization
26 Prepare
a detailed plan for defining, establishing, transitioning, and implementing an
independent Technical Engineering Authority, independent safety program, and a
reorganized Space Shuttle Integration Office as described in R7.5-1, R7.5-2,
and R7.5-3. In addition, NASA should submit annual reports to Congress, as part
of the budget review process, on its implementation activities. [RTF]
Recertification
27 Prior
to operating the Shuttle beyond 2010, develop and conduct a vehicle recertification
at the material, component, subsystem, and system levels. Recertification
requirements should be included in the Service Life Extension Program.
Closeout Photos/Drawing System
28 Develop
an interim program of closeout photographs for all critical sub-systems that
differ from engineering drawings. Digitize the close-out photograph system so
that images are immediately available for on-orbit troubleshooting. [RTF]
29 Provide
adequate resources for a long-term pro-gram to upgrade the Shuttle engineering
draw-ing system including:
• Reviewing drawings for accuracy
• Converting all drawings to a computer-aided drafting
system
• Incorporating engineering changes
o o
o
The Fate of Columbia's Crew
At the CAIB's request, NASA formed a Crew Survivability Working Group to determine, if possible, the cause of crew death. Here is what the group concluded (taken from page 77 of the Columbia Accident Investigation Report):
Medical and Life Sciences
The Working Group found no irregularities in its extensive review of all applicable medical records and crew health data. The Armed Forces Institute of Pathology and the Federal Bureau of Investigation conducted forensic analyses on the remains of the crew of Columbia after they were recovered. It was determined that the acceleration levels the crew module experienced prior to its catastrophic failure were not lethal. The death of the crew members was due to blunt trauma and hypoxia. The exact time of death sometime after 9:00:19 a.m. Eastern Standard Time cannot be determined because of the lack of direct physical or recorded evidence.
Failure of the Crew Module
The forensic evaluation of all recovered crew module/forward fuselage components did not show any evidence of over-pressurization or explosion. This conclusion is supported by both the lack of forensic evidence and a credible source for either sort of event. The failure of the crew module resulted from the thermal degradation of structural properties, which resulted in a rapid catastrophic sequential structural breakdown rather than an instantaneous "explosive" failure.
Separation of the crew module/forward fuselage assembly from the rest of the Orbiter likely occurred immediately in front of the payload bay (between Xo576 and Xo582 bulkheads). Subsequent breakup of the assembly was a result of ballistic heating and dynamic loading. Evaluations of fractures on both primary and secondary structure elements suggest that structural failures occurred at high temperatures and in some cases at high strain rates. An extensive trajectory reconstruction established the most likely breakup sequence, shown below (page 77 of the CAIB report).
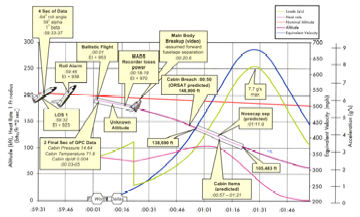
The load and heat rate calculations are shown for the crew module along its reconstructed trajectory. The band superimposed on the trajectory (starting about 9:00:58 a.m. EST) represents the window where all the evaluated debris originated. It appears that the destruction of the crew module took place over a period of 24 seconds beginning at an altitude of approximately 140,000 feet and ending at 105,000 feet. These figures are consistent with the results of independent thermal re-entry and aerodynamic models. The debris footprint proved consistent with the results of these trajectory analyses and models. Approximately 40 to 50 percent, by weight, of the crew module was recovered.
The Working Group's results significantly add to the knowledge gained from the loss of Challenger in 1986. Such knowledge is critical to efforts to improve crew survivability when designing new vehicles and identifying feasible improvements to the existing Orbiters.
Crew Worn Equipment
Videos of the crew during re-entry that have been made public demonstrate that prescribed procedures for use of equipment such as full-pressure suits, gloves, and helmets were not strictly followed. This is confirmed by the Working Group's conclusions that three crew members were not wearing gloves, and one was not wearing a helmet. However, under these circumstances, this did not affect their chances of survival.
o o
o
Reconstructed Timeline of Columbia's Re-entry
The following timeline was compiled by William Harwood, CBS News, from realtime telemetry and data from Columbia's recovered OEX recorder (through rev. 19 of NASA's internal entry timeline reconstruction), transcriptions of the NASA-Select commentary, mission control audio loops and portions of a 13-minute in-cabin video recovered after the accident.
The telemetry and OEX recorder data timing are exact, but the mission control audio and commentary entries are approximations. All such entries are tied to the assumption that shuttle commander Rick Husband's final transmission began at 8:59:32 a.m. EST, the moment the last valid data frame was transmitted from the orbiter. Likewise, the crew cabin comments by the astronauts were timed off on the assumption the tape began at exactly 8:35 a.m., which is the time NASA gave in a press release. The audio loop entries are believed accurate to within a few seconds.
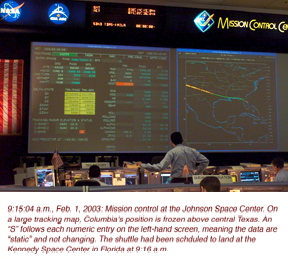 To
prevent interrupting the telemetry/mission control narrative, the NASA
commentator entries are presented in blocks, as they were spoken. Readers
should note, however, other events may be happening while the commentator is
talking, as reflected in the times listed for those events.
To
prevent interrupting the telemetry/mission control narrative, the NASA
commentator entries are presented in blocks, as they were spoken. Readers
should note, however, other events may be happening while the commentator is
talking, as reflected in the times listed for those events.
Many telemetry/OEX data entries include altitude in feet, Mach number and latitude and longitude in parentheses with north (+) latitude first followed by west (-) longitude, i.e., +36.398-150.847 means 36.398 degrees north latitude, 150.847 degrees west longitude. OEX data also reflect the number of seconds before and after entry interface, or EI, the moment Columbia reached the discernible atmosphere.
The timing of amateur video coverage of Columbia's re-entry is included in NASA's Master Timeline (rev. 19) and in the integrated timeline below. The start/finish times refer to actual footage, not when the shuttle rose above or passed below the horizon as viewed from the photographer's location. Each video entry includes the shooter's latitude and longitude in the same format discussed above.
Personnel mentioned:
MCC-FLIGHT - Entry flight director - LeRoy Cain, mission control center
MCC-CAPCOM - Astronaut Charles Hobaugh
MCC-FDO (Flight Dynamics Officer; pronounced "FIDO") - Richard Jones
MCC-INCO (Instrumentation and Communications Officer) - Laura Hoppe
MCC-MMACS (Maintenance, Mechanical, Arm and Crew Systems Officer) - Jeff Kling
MCC-GNC (Guidance, Navigation and Control Officer) - Mike Sarafin
MCC-GC (Ground Control Officer) - Bill Foster
MCC-GPO (Guidance and Procedures Officer) - Doyle Hensley
MCC-EECOM (Emergency, Environmental and Consumables Operation Manager) - Katie Rogers
MCC-LSO (Landing and Support Officer) - Martin Linde
MCC-MOD (Mission Operations Directorate Representative) - Phil Engelauf
MCC-Commentator - James Hartsfield, NASA/JSC public affairs officer
STS-A/G (Shuttle Commander, air-to-ground audio) - Shuttle commander Rick Husband, aboard Columbia
STS-ICOM - Indicates cockpit intercom voice traffic captured on in-cabin video
Shuttle Columbia's Final Re-Entry: A Voyage into History
Flying upside down and backward over the Indian Ocean, commander Rick Husband and pilot William "Willie" McCool fired Columbia's twin orbital maneuvering system braking rockets at 8:15:30 a.m. EST to begin the shuttle's long glide back to Earth. There were no signs of any technical problems and the weather at the Kennedy Space Center was improving after initial concerns about cloud cover.
Columbia fell into the discernible atmosphere 400,000 feet above the Pacific Ocean northwest of Hawaii at 8:44:09 a.m. Re-entry was normal until 8:48:39 a.m. when a strain gauge in the shuttle's left wing began showing an unusual increase. Twenty seconds later, a temperature sensor in the left wing's leading edge began showing an off-nominal increase as hot gas shot into a cavity behind the U-shaped reinforced carbon carbon panels making up the leading edge.
Additional left wing sensors soon began registering elevated temperatures and data from a series of sensors across the back of the left wing simply stopped flowing. At almost the same time, Columbia's flight control system began sensing unexpected aerodynamic drag on the left side of the spacecraft and commands were sent to adjust the shuttle's roll trim using the elevons at the back of each wing. This unusual drag steadily worsened as Columbia streaked across the southwestern United States.
It now appears a breach in the shuttle's wing, on the lower side of reinforced carbon carbon panel No. 8, allowed a plume of hot plasma to enter the wing structure. The wiring for the failed sensors at the back of the wing was routed just to the left and then in front of the left main landing gear wheel well. Analyses and testing on the ground show a breach in RCC panel 8 is the most likely explanation for what happened during Columbia's re-entry.
That said, here is a timeline of the final hour of Columbia's 28th flight.
08:10:39 a.m. - TIG-5 minutes: APU-2 startup.
08:15:30 a.m. - TIG-0: Deorbit ignition. Change in velocity: 176 mph; Burn duration: two minutes and 38 seconds. Location (latitude/longitude in minutes:seconds): -33:35+98:10; altitude: 175.95 statute miles. Velocity: 17,319.7 mph
08:18:08 a.m. - Deorbit burn complete.
08:26:09 a.m. - Forward reaction control system propellant dump begins.
08:27:12 a.m. - FRCS dump complete.
08:31:25 a.m. - APU-1 startup. Entry interface (EI) minus 13 minutes.
08:31:29 a.m. - EI-760 seconds - APU-3 startup.
08:31:57 a.m. - EI-732 - APU-1 at normal operating pressure.
08:31:59 a.m. - EI-730 - APU-2 at normal operating pressure.
08:32:01 a.m. - EI-728 - APU-3 at normal operating pressure.
08:32:29 a.m. - EI-700 - Shuttle main engine stow sequence begins (thrust vector control system isolation valve 1 to close).
08:39:09 a.m. - EI-300. Transition to OPS-304 software load; aerojet digital autopilot and entry guidance are activated; open-loop guidance (angle of attack = 40 degrees, roll angle = 0 degrees). Mach: 24.40.
08:39:11 a.m. - EI-298 - Speedbrake closed; rudder commanded to zero degrees.
08:39:28.559 a.m. - EI-280.4 - OEX: Start of pulse code modulation - PCM - data block.
Editor's note: For clarity, mission control audio and cockpit voice loops have been omitted to this point. All conversations were normal and thus have no significance to the accident investigation. We pick up the timeline roughly two minutes before entry interface, the point where the shuttle enters the discernible atmosphere 400,000 feet above the Pacific Ocean.
08:41:35 a.m. - STS-ICOM: Commander Rick Husband: "Two minutes to entry interface."
08:41:43 a.m. - STS-ICOM: Laurel Clark: "I know about the line cable, Willie, I didn't understand your question. You don't want the camera back, right?"
08:41:51 a.m. - STS-ICOM: Pilot William "Willie" McCool: "I do not want the camera back.
STS-ICOM: Husband: "He's got one mounted in his HUD already."
STS-ICOM: Clark: OK. Yep, yep, yep. Yep, Replug."
08:41:54 a.m. - MCC-Commentator: "This is mission control, Houston. Columbia's altitude is now 90 miles above the Pacific Ocean to the north of the Hawaiian islands, about two minutes away from entering the Earth's atmosphere. All activities continuing to go smoothly en route toward a touchdown at the Kennedy Space Center at 8:16 a.m. Central time."
08:41:58 a.m. - STS-ICOM: McCool: "Replug, that's all you've gotta do."
08:42:08 a.m. - STS-ICOM: McCool: "When do we start moving our head around, Rick? When we start getting a little bit of Gs?"
STS-ICOM: Husband: "A little bit of Gs, yeah."
08:42:29 a.m. - STS-ICOM: Clark (operating a video camera): "KC, can you look at the camera a second? Look at me."
08:42:35 a.m. - STS-ICOM: Flight engineer Kalpana Chawla: "Me?"
STS-ICOM: Clark: Yep. Yeah. What KC?"
08:42:37 a.m. - MCC-Commentator: "Columbia is currently targeted toward runway three-three at the Kennedy Space Center, the runway selection continues to be discussed here in mission control, however. But for its approach to runway three-three, Columbia will perform a right overhead turn to align with the runway of about 214 degrees around the heading alignment cylinder, an imaginary cylinder created by the microwave landing system for the shuttle that assists in guiding it for its final approach."
08:42:38 a.m. - STS-ICOM: Chawla: "Oh, I just turn towards you, I see what you have there."
STS-ICOM: Clark: "Yeah." (laughter)
STS-ICOM: Chawla: "OK, Laurel."
08:42:51 a.m. - STS-ICOM: McCool: "Trash bag, KC, if you've got any."
STS-ICOM: Chawla: "We are gray taping, you can just give it to us."
08:42:57 a.m. - STS-ICOM: McCool: "That's six and a half bags."
STS-ICOM: Chawla: "OK, I'm going to have to give this to Laurel when she is done."
08:43:05 a.m. - STS-ICOM: Chawla: "I'm going to gray tape it behind, I mean (garble) tape it behind the seat, I think this is light enough that it will stay."
08:43:18 a.m. - STS-ICOM: McCool: "Laurel, you see lots of jets firing."
STS-ICOM: Clark: "I'm getting the jets firing, I'm trying to see if I can get an overhead window view yet."
08:43:25 a.m. - STS-ICOM: Husband: "OK. That's all I can do is three and a half bags out of four. So that'll work. If I can pass that back to you?"
08:43:32 a.m. - STS-ICOM: Chawla: "Rick, if you could wait just one second, I want to get to my gloves before Gs build, I don't want to get..."
STS-ICOM: Husband: "Certainly."
STS-ICOM: Chawla: "...two up."
STS-ICOM: Husband: "Certainly."
08:43:40 a.m. - STS-ICOM: Chawla: "Here comes (garble)."
08:43:42 a.m. - STS-ICOM: Husband: "OK. We're just past EI."
STS-ICOM: Clark: "Ok."
STS-ICOM: Chawla: "I have both gloves."
08:43:47 a.m. - STS-ICOM: Clark: "Is that jets firing on the DAP, I guess."
STS-ICOM: Chawla: "And Rick, I'll take your bag. And float it aft gently, I've got it."
08:43:58 a.m. - STS-ICOM: McCool: "That might be some plasma now."
STS-ICOM: Clark: "Think so, already?"
STS-ICOM: McCool: "Yeah, the jets are not firing right now."
STS-ICOM: Clark: "All right, it was quite a (GARBLE), actually."
STS-ICOM: McCool: "We see it out the front, also."
STS-ICOM: Husband: "That's some plasma."
08:44:09 a.m. - EI+0 - Actual moment of entry interface. The shuttle falls into the discernible atmosphere 395,010 feet over the Pacific Ocean at a velocity of Mach 24.57 (+30.833-167.556).
08:44:09 a.m. - STS-ICOM: Clark: "Copy, and there's some good stuff outside. I'm filming overhead right now."
STS-ICOM: McCool: "It's kind of dull."
STS-ICOM: Husband: "Oh, it'll be obvious when the time comes."
08:44:18 a.m. - STS-ICOM: Clark: "Well, Willy, I guess I could give you the camera to put out the front window."
STS-ICOM: Husband: "Here, let's, uh, no, let's don't do that."
STS-ICOM: Clark: "OK."
STS-ICOM: Husband: "Let's just, uh, let's go ahead and make sure you check your suit pressure integrity, too."
STS-ICOM: Clark: "All right."
08:44:51 a.m. - STS-ICOM: Husband: "And comm check on intercom. Put the, uh, visors down. CDR."
STS-ICOM: McCool: "PLT."
STS-ICOM: Clark: "PS1. (then laughing to correct herself) MS1."
STS-ICOM: Chawla: "I don't have my gloves on yet. MS2."
STS-ICOM: Husband: "All right, good enough."
08:45:09 a.m. - STS-ICOM: Clark: "And we're going to leave visors down, though."
STS-ICOM: Husband: "Oh, no. I'm just saying just check your suit's..."
STS-ICOM: Clark: "OK."
STS-ICOM: Husband: ".. pressure."
STS-ICOM: Clark: "And then I'm going to go back off. Yeah."
STS-ICOM: Husband: "Yeah."
08:45:16 a.m. - MCC-Commentator: "Columbia's altitude now 71 statute miles as it enters Earth's atmosphere above the Pacific Ocean en route to the Kennedy Space Center, its speed 17,000 miles per hour."
08:45:20 a.m. - STS-ICOM: Husband: "That's good enough for (GARBLE), I'm going to check one other thing."
08:45:32 a.m. - STS-ICOM: McCool: "Starting to glow a little bit more now, Laurel."
STS-ICOM: Husband: "Yeah... OK, all that's worked."
08:45:39-48:59 a.m. - OEX data: 16 temperature sensors on the lower surface to the left of, or on, the vehicle centerline show off-nominal early temperature trends (warmer rise rate compared to previous flights by Columbia). EI+90-290.
08:45:42 a.m. - MCC-Commentator: "Columbia with wings level and nose angled up at about 40 degrees to control heating as it descends into the atmosphere. It's altitude now 68 miles. As Columbia descends into the atmosphere and approaches the continental United States it'll perform the first in a series of four banks it performs as it approaches the Kennedy Space Center. That first bank to the right, then back to the left, then back to the right and then a final bank to the left as it approaches Kennedy and the Shuttle Landing Facility runway. Those designed to dissipate speed for the shuttle as it descends into the atmosphere toward landing."
08:45:49 a.m. - STS-ICOM: Husband: "It's noisy in there, isn't it?
08:45:52 a.m. - STS-ICOM: McCool: "Do see it over my shoulder now, Laurel?"
STS-ICOM: Clark: "I was filming, it doesn't show up nearly as much as the back."
08:45:58 a.m. - STS-ICOM: McCool: "It's going pretty good, now. Ilan, it's really neat, just a bright orange yellow out over the nose, all around the nose."
08:46:10 a.m. - STS-ICOM: Husband: "Wait until you start seeing the swirl patterns out your left and right windows."
STS-ICOM: McCool: "Wow."
STS-ICOM: Husband: "Looks like a blast furnace."
08:46:12 a.m. - FDO: FLIGHT, FIDO.
08:46:31 a.m. - STS-ICOM: Husband: "Let's see here... look at that.
STS-ICOM: McCool: "Yep, we're getting some gees.
STS-ICOM: Husband: "Yeah."
STS-ICOM: McCool: "I let go of a card, and it falls."
08:46:26 a.m. - MCC-FLIGHT: "OK, FDO, go ahead."
MCC-FDO: "This data set is a spliced data set. This is my back room's attempt to, uh, get us some data off that first balloon that was broken. And it shows us 11 hundred 60 feet at the close-in aim point."
MCC-FLIGHT: "With the close..."
MCC-FDO: "Yes sir. And we're waiting for our re-release balloon, which was just released a few minutes ago."
MCC-FLIGHT: "OK. Now, uh, we lost the balloon at 6,000 feet and, did we get it back at some point? Or when you say 'spliced it together,' I mean, I don't want, I don't know whether I should..."
08:46:30 a.m. - MCC-Commentator: "Just under 30 minutes to touchdown for Columbia now, altitude 64 miles."
08:46:39 a.m. - STS-ICOM: McCool: I got a bit flip here on the accel now."
08:46:48 a.m. - Qbar equals 0.5 pounds per square foot. Mach: 24.66
STS-ICOM: Husband: "Yep. Alright, we're at, uh, hundredth of a G."
08:46:51 a.m. - STS-ICOM: McCool: "This is amazing, it's really getting, uh, fairly bright out there."
08:46:56 a.m. - STS-ICOM: Husband: "Yep. Yeah, you definitely don't want to be outside now."
08:47:00 a.m. - MCC-FDO: "We did not, we did not get any data beneath 6K, I mean above 6K, excuse me...
08:47:01 a.m. - STS-ICOM: Chawla: "What, like we did before?
STS-ICOM: (laughter)
08:47:03 a.m. - MCC-FLIGHT: "OK."
MCC-FDO: "... and we spliced basically a previous data set..."
MCC-FLIGHT: "I got you."
MCC-FDO: "... on top of this one to give us an estimate."
08:47:03 a.m. - STS-ICOM: McCool: "How's it look out the back, Laurel?"
STS-ICOM: Husband (responding to Chawla): "Good point."
STS-ICOM: Clark: "Uh..."
08:47:09 a.m. - STS-ICOM: Clark(?): "Willie, I can see you in your mirror."
STS-ICOM: McCool: "Not yet?"
08:47:11 a.m. - MCC-FLIGHT: "Now let's see, from where we're releasing the balloons to, which way... are they going out over the water with the wind direction from the surface on up to about 10,000 feet, the direction is roughly out of the west, isn't it?"
MCC-FDO: "Yes, flight, they are going out the water, out over the water, I concur with that, we are..."
MCC-FLIGHT: "We start out with them far enough away from where our HAC really is and then they're going the wrong way."
08:47:14 a.m. - STS-ICOM: Clark: "Not, not, yeah, now I can.
STS-ICOM: McCool: "Now I can see your camera."
STS-ICOM: Husband: "OK." (said as if to tell the crew it's time to start paying attention)
08:47:19 a.m. - STS-ICOM: Clark: "Stop playing."
08:47:20 a.m. - STS-ICOM: Chawla: "I see 22-10. 10-52 is what we were looking for, for...
STS-ICOM: Husband: "OK. 10-16, right? I've got 16 written here."
08:47:32 a.m. - STS-ICOM: McCool: "Yeah, 22 10 16."
STS-ICOM: Chawla: "Yeah, 22 10 16, that's correct. Sorry."
Editor's Note: The ICOM video tape ends at this point.
08:47:38 a.m. - MCC-FDO: "I would concur, we are seeing, we're definitely seeing some spatial differences here. From the STA (shuttle training aircraft) and this morning. I would concur with that."
MCC-FLIGHT: "OK, well yeah, and the STA, the last dive here - and we're not going to have him do any more - was 19 41 (1,941 feet) with close."
MCC-FDO: "Ummm"
08:47:48 a.m. - MCC-Commentator: "Columbia's course toward Florida will take it across the continental United States, crossing the California coast above the San Francisco bay area and continuing across Sacramento, California, providing a spectacular view for persons in that area of Columbia's descent through the atmosphere. That observation of the shuttle would begin about 5:51 a.m. Pacific standard time and continue for about four minutes, until about 5:55 a.m. Pacific time, with the shuttle at an elevation of about 78 degrees."
08:47:52 a.m. - EI+223 - QBAR = 2.0 psf; elevons and body flap are now available for attitude control. H=288,932; Mach: 24.66 (+36.398-150.847)
08:47:55 a.m. - MCC-FLIGHT: "He normalized to 19 41 with close."
MCC-FDO: "Yeah..."
MCC-FLIGHT: "Did I get that right?"
MCC-FDO: "X-corrected I heard was 17 84. The X-corrected normalized."
08:48:09 a.m. - MCC-FLIGHT: "Yeah, we're talking about the normalized."
MCC-FDO: "I think the STA performs a correction on top of the normalization to account for, ummm,
MCC-FLIGHT: "Yeah, you're talking XCN, I was just saying the normalized is 19 41."
MCC-FDO: "Yes sir."
08:48:15 a.m. - MCC-Commentator: "It'll be visible as well through much of the United States' southwest above southern Nevada and northern Arizona and central Mexico as it continues its descent through the atmosphere, trailing a plasma trail left as it heats the atmosphere around it during its descent.
08:48:24 a.m. - MCC-FLIGHT: "OK, what we've got, the last balloon data to come in before we make our decision."
MCC-FDO: "Yes sir."
08:48:39 a.m. - EI+270 - OEX: Strain gauge sensor V12G9921A, located inside left wing in line with RCC panel No. 9, begins to show a small but off-nominal increase. Sensor fails at EI+495 seconds. This is the first indication of anything amiss aboard Columbia.
08:48:40 a.m. - MCC-Commentator: "Columbia's altitude now 54 miles as it continues to descend into the atmosphere, wings level, nose angled up 40 degrees to control heating. Columbia's traveling about 17,000 miles per hour."
08:48:59 a.m. - EI+290 - OEX: Temperature sensor VO9T9910A mounted on the lower attach clevis between RCC 9 and 10 begins showing an off-nominal increase. This is the first sign of unusual heating. This sensor begins to fail at EI+492 seconds.
08:49:07 a.m. - EI+298 - Entry guidance begins closed loop roll control to converge aerodynamic drag to the reference drag profile. H=259,978; Mach: 24.58 (37.639-144.803)
08:49:16 a.m. - EI+307 - Roll jets deactivated. Qbar equals 10 pounds per square foot. From this point on, roll control is achieved through aileron positioning and yaw jet firings. Mach: 24.57
08:49:32 a.m. - EI+323 - Initial roll. Entry guidance software determines a non-zero roll is required to achieve desired drag level. Mach 24.51.
08:49:38 a.m. - MCC-GPO: "CLG (closed loop guidance) init."
MCC-FLIGHT: "Copy."
08:49:39 a.m. - EI+330 - OEX: Left wing front spar strain gauge V12G9169A shows early off nominal downward trend (trend may have started slightly earlier).
08:49:49-59 a.m. - EI+340/350 - OEX: Four left OMS pod sensors (VO7T9976A, VO7T9220A, VO7T9978A, VO7T9972A) start an off-nominal temperature trend, a cooler rise rate than previous flights followed by a large increase at EI+520 seconds.
08:50:03 a.m. - MCC-GPO: "Rolling right."
08:50:00 a.m. - EI+351 - Qbar about 15 psf; Mach 24.4; wing leading edge stagnation temperature about 2,520 degrees Fahrenheit.
08:50:00-43 a.m. - EI+351/394 - Five unexpected return link S-band communications drop outs; upper left aft antenna/TDRS-171 West. Out of family based on comparison with previous Columbia entries from 39-degree inclination orbits to KSC and similar look angles to TDRS West.
08:50:03 a.m. - MCC-Commentator: "Columbia's altitude 48 statute miles as it begins the first in a series of four banks to dissipate speed as it descends into the atmosphere, banking to the right now, a steep bank of 60 degrees and approaching the west coast of the United States. Columbia's speed 16,620 miles per hour, range to touchdown at the Kennedy Space Center runway 3,450 statute miles."
08:50:06 a.m. - STS-?: "garble in static"
08:50:09 a.m. - EI+360 - OEX: Left payload bay door surface temperature sensor V07T9925A starts an unusual trend, a cooler rise rate than previous flights followed by a large increase at EI+570 seconds.
08:50:19 a.m. - EI+370 - OEX: Left wing lower surface temperature sensor begins off-nominal increase from about 2,000 degrees to 2,200 degrees over 50 seconds followed by a short 100-degree temperature spike. Sensor fails at EI+496.
08:50:26 a.m. - MCC-MALE VOICE: "I got it."
08:50:30 a.m. - EI+381 - First indication of re-entry heating in downlinked telemetry; nominal rise in aft fuselage center bottom line bond temperature sensor.
08:50:53 a.m. - EI+404 - Start of peak heating region; this is the region during which the heating rate has stabilized at or near its maximum value. H=243,048; Mach: 24.12 (+38.744-136.142)
08:50:56 a.m. - MCC-Commentator: "Columbia in almost an 80-degree-bank to the right to dissipate speed, the first of four banks it performs as it approaches Florida to slow down as it descends. Altitude now 47 miles or about 248,000 feet. The shuttle's speed is 16,400 miles per hour."
08:51:14 a.m. - EI+411 - Qbar about 19 psf; Mach 24.1; wing leading edge stagnation temperature: 2,650 degrees.
08:51:14 a.m. - EI+425 - OEX: Temperature sensor V09T9895A, located inside the left wing roughly in line with RCC panel No. 9, begins showing an unusual temperature increase. This indicates a plume of hot gas has entered the wing's interior through a breach in the leading edge. Measurement fails at EI+520.
08:51:14 a.m. - EI+425 - OEX: Left wing temperature sensor V09T9910A at RCC panel 9 lower attach clevis (between RCC 9 and 10) begins a rapid increase. Measurement fails at EI+492.
08:51:26 a.m. - MCC-Commentator: "Aboard the shuttle on the flight deck are shuttle commander Rick Husband and pilot Willie McCool, flight engineer Kalpana Chawla and mission specialist Laurel Clark. On the lower deck of the shuttle for entry are payload commander Mike Anderson, mission specialist David Brown and payload specialist, from the Israel space agency, Ilan Ramon."
08:51:49 a.m. - EI+460 - OEX: Left OMS pod HRSI surface temperature sensor V07T9223A begins a higher-than-expected temperature trend.
08:13:52 a.m. - EI+471 - Qbar = 22 psf; Mach 23.7; wing leading edge stagnation temperature = 2,700 degrees.
08:52:05 a.m. - MCC-Commentator: "Columbia approaching the Coast of California now, it is predicted to cross the coast and be visible in the San Francisco area about 5:51 a.m. Central time, uh, Pacific standard time rather, and pass almost directly overhead of Sacramento, California. It actually crosses the California coast just to the north of the San Francisco area."
08:52:09-15 a.m. - EI+480/486 - Sixth unexpected S-band return link comm dropout. Out of family based on previous flight data.
08:52:09-49 a.m. - EI+480/520 - OEX: Nose cap RCC chin panel temperature sensor V09T9889A exhibits a temporary change in slope then returns to normal. An adjacent sensor shows no change.
08:52:15 a.m. - EI+486 - Second indication of normal entry heating in downlinked telemetry; nominal rise in center line bond temperature sensor (2). Mid fuselage "mid" skin temperature; mid fuselage bottom center bond line temperature at x1214.
08:52:16 a.m. - EI+487 - OEX: Two left wing and one right wing surface pressure measurements begin showing signs of failure. This is the first data on the OEX tape to show signs of failure.
08:52:16-53:17 a.m. - EI+487/522 - OEX: All active measurements (except PCM snapshot data) routed through wire bundles along the left wing leading edge begin to show signs of failure. Eighteen measurements in all.
08:52:16-56:24 a.m. - EI+487/735 - OEX: Nearly all left wing OEX measurements show signs of failure during this period, including all left wing temperature and pressure measurements and all strain gauge data aft of Xo 1040 with exception of three on the upper surface of the main landing gear wheel well. In addition, 30 right wing pressure measurements begin showing signs of failure.
08:52:17 a.m. - Approximate vehicle location as first signs of off-nominal telemetry were received on the ground: 300 miles from the California coast. H=236,800; Mach: 23.6 (+39.0-129.2).
08:52:17 a.m. - Left main gear brake temperature D sensor on wheel well sidewall aft of switch valves shows a one "bit flip" change, indicating an increase of about 1.5 degrees. This reading initially was believed to be the first sign of off-nominal heating inside the left wing but it may, in fact, have been normal. NASA research shows at least 13 other missions saw similar bit flips in the same time frame. H=236,791; Mach: 23.58 (+38.993-129.151)
08:52:18 a.m. - EI+489 - OEX: Left wing lower spar cap strain gauge shows an unusual increase followed by a gradual decrease over 330 seconds until the measurement fails at EI+935.
08:52:21-24.8 a.m. - EI+492/495.8 - OEX: Two left wing temperature sensors begin an off-nominal response that appears to be an indication of wiring damage. Temperature sensor V09T9910A, located in front of the left wing spar behind RCC panel 9, drops off line after climbing to 50 degrees Fahrenheit. This sensor was insulated and presumably dropped off-scale low when its wiring was damaged or severed by hot gas.
08:52:22 a.m. - EI+493 - OEX: Unusual temperature shifts from five temperature sensors on a common power circuit.
08:52:24 a.m. - EI+495 - OEX: Left wing front spar RCC 9 strain gauge goes erratic for 20 seconds; appears to be failing at this point.
08:52:25 a.m. - EI+496 - OEX: left outboard elevon wide band accelerometer shows unusual vibration response of 2Gs, peak to peak. V08D9729A.
08:52:25-31 a.m. - EI+496/502 - Unexpected S-band return link comm drop outs (events 7 and 8).
08:52:29 a.m. - EI+500 - OEX: Approximately 10 percent of the strain gauges in the right wing show a small but unusual data trend; signal "flattens" followed by normal data increase or an increase in strain.
08:52:29 a.m. - EI+500 - OEX: Left wing surface temperature sensor V07T9674A begins showing an 80-degree drop over 20 seconds.
08:52:29 a.m. - EI+500 - OEX: Left OMS pod surface temperature sensor V07T9219A begins a slightly off-nominal erratic trend.
08:52:31 a.m. - EI+502 - OEX: Left outboard elevon wide-band accelerometer shows an unusual vibration (3Gs peak to peak).
08:52:31.3-38.4 a.m. - EI+502.3/509.4 - OEX: Five left wing temperature sensors begin off-nominal trends indicative of wiring failures (sensors in the group first mentioned at 8:52:16 a.m.
08:52:32 a.m. - EI+503 - Supply water dump nozzle temperature sensors A and B show temporary increase in temperature rise rate (15-second duration), then return to normal profile. Vacuum vent temperature shows temporary increase in rise rate (23 seconds) then returns to normal profile. H=235,602; Mach: 23.47 (+38.974-127.894)
08:52:34 a.m. - EI+505 - OEX: Left OMS pod HRSI temperature sensor V07T922A begins lower than expected trend until a sharp increase at EI+910; goes erratic at EI+940.
08:52:39-53:09 a.m. - EI+510/540 - OEX: Four left OMS pod surface temperature sensors showing a cooler rise rate than expected suddenly begin trending upward.
08:52:41 a.m. - EI+512 - Left main gear brake line temperature A sensor on strut facing the main landing gear door begins seeing an off-nominal temperature rise; left main gear brake line temperature sensor C sees off-nominal temperature rise. H=234,928; Mach: 23.40 (+38.995-127.191)
08:52:44-50 a.m. - EI+515/521 - First clear indication of off-nominal aero increments (delta yawing moment coefficient goes off nominal at 8:52:44 a.m.; delta rolling moment coefficient goes off nominal at 8:52:50 a.m.).
08:52:47 a.m. - EI+518 - Supply water dump nozzle temperature sensors A and B return to normal rise rate.
08:52:49-55 a.m. - EI+520/526 - Unexpected S-band return link comm dropout (event 9).
08:52:49.5-51.4 a.m. - EI+520.5/522.4 - OEX: Two left wing temperature sensors - V09T9895A, located inside the left wing behind RCC panel 9, and V09T9849A, outboard elevon lower surface edge - begin failing due to wiring damage.
08:52:54 a.m. - MCC-Commentator: "Columbia is on target for runway three-three at the Kennedy Space Center Shuttle Landing Facility runway."
08:52:55 a.m. - EI+526 - Vacuum vent temperature sensor returns to normal rise rate.
08:52:56 a.m. - EI+527 - Left inboard elevon lower skin temperature sensor starts an off-nominal trend downward.
08:52:59 a.m. - EI+530 - Left inboard elevon lower skin temperature goes off-scale low (drops off line). H=233,618; Mach: 23.25 (+38.895-125.714)
08:52:59.4-53:07.4 a.m. - EI+530.4/538.4 - OEX: Five left wing temperature sensors begin to show signs of wiring failure.
08:53:00 a.m. - EI+531 - Qbar = 25.5 psf; Mach 23.2; wing leading edge stagnation temperature = 2,800 degrees.
08:53:00 a.m. - MCC-Commentator: "The subject of runway selection has been discussed in mission control, it continues to be discussed some, but in the meanwhile at present the original targeting for Columbia is toward runway three-three..."
08:53:02 a.m. - EI+533 - Hydraulic system 1 left inboard elevon actuator return line temperature begins trending down; Hydraulic system 3 left outboard elevon return line temperature sensor begins trending down. H=233,457; Mach: 23.23 (+38.883-125.482)
08:53:03 a.m. - EI+534 - OEX: Left outboard elevon wide-band accelerometer exhibits signal saturation indicative of failure (10 Gs peak to peak).
08:53:10 a.m. - "... and as it approaches runway three-three, it will perform a right overhead 212-degree turn to align with that runway around the heading alignment cylinder, an imaginary cylinder created by the microwave scan beam landing system at the shuttle runway that assists in the shuttle's guidance toward its final approach to the runway."
08:53:10 a.m. - Hydraulic system 3 left outboard elevon return line temperature sensor drops off-scale low (preceded by nominal temperature rise). H=232,864; Mach: 23.17 (+38.848-124.864)
08:53:11 a.m. - Hydraulic system 1 left inboard elevon actuator return line temperature sensor goes off-scale low (preceded by nominal temperature rise). H=232,793; Mach: 23.16
08:53:15 a.m. - EOC2-4-0064/Fairfield, California: Video coverage begins. (Lat/Lon TBD)
08:53:26 a.m. - Columbia crosses the California coastline. H=231,600; Mach: 23.0 (+38.7-123.5)
08:53:29 a.m. - EOC2-4-0056/Lick Observatory, California: Video coverage begins. (+37.342-121.643)
08:53:29 a.m. - EI+560 - OEX: Left fuselage side surface temperature sensor V07T9253A begins an off-nominal increase, jumping from 180 degrees to 400 degrees.
08:53:29 a.m. - EI+560 - OEX: Left payload bay door surface temperature sensor V07T9913A starts a slightly off-nominal erratic trend.
08:53:29 a.m. - EI+560 - OEX: Left payload bay door surface temperature sensor V0T9925A begins an unusual rise, peaking at EI+625, followed by a temperature drop and subsequent increase.
08:53:29 a.m. - EI+560 - OEX: Left fuselage side surface temperature sensor V07T9903A starts a slightly off-nominal erratic trend.
08:53:31 a.m. - EI+562 - Entry guidance enables limited change in angle of attack (alpha modulation) to help vehicle converge on desired drag profile.
08:53:31-34 a.m. - EI+562/565 - Hydraulic system 1 left outboard elevon return line temperature drops off-scale low. Preceded by normal temperature rise; data loss three seconds prior to event. H=231,304; Mach: 23.0
08:53:32 a.m. - MCC-Commentator: "Shuttle's altitude now 45 miles, speed 15,800 miles per hour, continuing in a right bank with wings angles 70 degrees, the first of four banks it performs to dissipate speed as it approaches landing."
08:53:32-34 a.m. - EI+563/565 - Unexpected S-band return link comm drop out (event 10).
08:53:34-55:57 a.m. - EI+565/668 - Third indication of re-entry heating in downlinked telemetry with nominal rise in three center line bond temperature sensors (mid fuselage bottom port bondline temps x620, x777 and forward fuselage lower skin bottom center line).
08:53:34 a.m. - EI+565 - Hydraulic system 2 left inboard elevon return line temperature begins trending down. H=231,077; Mach: 22.97 (+38.707-122.952)
08:53:36 a.m. - EI+567 - Hydraulic system 2 left inboard elevon return line temperature goes off-scale low. H=230,915; Mach 22.95
08:53:36 a.m. - EOC2-4-0026/Sparks, Nevada: Video coverage begins. (+39.541-119.768)
08:53:37 a.m. - EI+568 - OEX: Main landing gear forward spar wall strain gauge begins showing an unusual increases over a 115-second period followed by a sudden decrease.
08:53:38 a.m. - EI+569 - Inertial sideslip angle (beta) goes negative and stays negative until loss of signal; consistent with a negative rolling and yawing torque on the spacecraft.
08:53:44 a.m. - EI+575 - OEX: Left OMS pod HRSI surface temperature sensor begins an off-nominal lower-than-expected trend; goes erratic at EI+940.
08:53:45-47 a.m. - EI+576/578 - Debris No. 1: First report of debris observed leaving the orbiter. Seen just behind orbiter envelope. No evidence of RCS thruster firing. H=230,348; Mach: 22.88 (+38.631-122.119)
08:53:45 a.m. - MCC-Commentator: "Columbia crossing the California coast, again, just to the north of the San Francisco area. It's course will take it across Sacramento, California."
08:53:46-50 a.m. - EI+577/581 - Debris No. 2: Second report of debris observed leaving the orbiter, just aft of the shuttle envelope. No evidence of RCS thruster firing. H-=230,276; Mach: 22.87 (+38.624-122.044)
08:53:46 a.m. - EI+577 - Left main gear brake line temperature A sensor on strut facing main landing gear door begins showing a rise from 1.4 degrees Fahrenheit per minute to 5.5 F/min; increases through loss of signal. H=230,203; Mach: 22.86 (+38.616-121.968)
08:53:47.6 a.m. - EI+578.6 - OEX: Another left wing temperature sensor begins off-nominal response that appears to be related to wiring damage.
08:53:54-58 a.m. - EI+585/589 - Debris No. 3: Third report of debris shedding, directly above Sacramento. Seen just aft of the shuttle. Momentary brightening of plasma trail. No evidence of RCS thruster firings. H=229,621; Mach: 22.79 (+38.554-121.367)
08:54:00 a.m. - EI+591 - Qbar = 29 psf; Mach 22.7; wing leading edge stagnation temperature = 2,850 degrees.
08:54:00-04 a.m. - EI+591/595 - Debris No. 4: Fourth report of debris shedding just east of Sacramento, seen just aft of the orbiter. No evidence of RCS thruster firings. H=229,113; Mach: 22.73 (+38.496-120.843)
08:54:03 a.m. - EOC2-4-0034/Reno, Nevada: Video coverage begins. (+39.53-119.813)
08:54:07-11 a.m. - EI+598/602 - Debris No. 5: Fifth report of debris shedding; seen just aft of orbiter envelope. No evidence of RCS thruster firings. H=228,817; Mach: 22.69 (+38.461-120.545)
08:54:10 a.m. - EI+601 - Left main gear brake line temperature B sensor begins showing an off-nominal temperature rise. H=228,460; Mach: 22.64 (+38.416-120.172)
08:54:11 a.m. - EI+602 - Roll moment coefficient changes from negative to positive, indicating lift acting on the left wing.
08:54:14-22 a.m. - EI+605/613 - Unexpected S-band return link comm drop out (event 11).
08:54:15 a.m. - EOC2-4-0009-B/Springfield, California: Video coverage begins. (+36.226-118.805)
08:54:18 a.m. - EOC2-4-0064/Fairfield, California: Video coverage ends. (Lat/Lon TBD; exact LOS time TBD)
08:54:20 a.m. - EI+611 - Start of slow elevon trim change to counteract the buildup of aerodynamic drag on the left wing. (Time approximate; +/- 10 seconds)
08:54:22 a.m. - EI+613 - Mid fuselage left bondline temperature sensor at x1215 begins reporting an unusual rise from 1 F/min to 7.5 F/min; Left aft fuselage sidewall temperature sensor at x1410 begins seeing an unusual increase from 2.7 F/min to 5.4 F/min. H=227,560; Mach: 22.52
08:54:24 a.m. - EI+615 - System 3 left main gear strut actuator temperature sensor begins reporting an off-nominal temperature increase. H=227,437; Mach: 22.51 (+38.270-119.068)
08:54:24 a.m. - MCC-MMACS: "Flight, MMACS."
MCC-FLIGHT: "Go ahead, MMACS."
MCC-MMACS: "FYI, I've just lost four separate temperature transducers on the left side of the vehicle, hydraulic return temperatures. Two of them on system one and one in each of systems two and three.
08:54:25 a.m. - EI+616 - Columbia crosses the California-Nevada state line. H=227,400; Mach: 22.5 (+38.3-119.0)
08:54:26 a.m. - EI+617 - S-band comm switched from upper left antenna to upper right antenna. Nominal event.
08:54:28 a.m. - EOC2-4-0056/Lick Observatory, California: Video coverage ends. (+37.342-121.643)
08:54:29 a.m. - EI+620 - OEX: Left fuselage side surface temperature sensor V07T9253A peaks and begins a downward trend.
08:54:33 a.m. - EOC2-4-0030/Las Vegas, Nevada: Video coverage begins. (+36.309-115.274)
08:54:33.3-33.9 a.m. - EI+624.3/624.9 - Flash No. 1: Orbiter envelope suddenly brightened for 0.3 seconds, leaving "noticeably luminescent" signature in Columbia's plasma trail. R3R and R2R thrusters fired briefly at 8:54:33.52 and .76 respectively and again at 8:54:33.54 and 78). H=226,894; Mach: 22.43
08:54:34 a.m. - EI+625 - OEX: Left fuselage side surface temperature sensor V07T9925A peaks and begins downward trend.
08:54:35-37 a.m. - EI+626/628 - Debris No. 6: Sixth report of debris leaving the shuttle; described as "very bright." Orbiter envelope brightened for 0.3 seconds. Debris events 6 and 14 are visually the brightest of all such events over the western United States. H=226,748; Mach: 22.41 (+38.154-118.265)
08:54:39 a.m. - EI+630 - OEX: Strain gauges on the upper surface of the left main landing gear wheel well show higher-than-expected strains.
08:54:39 a.m. - EI+630 - OEX: Left wing x1040 spar shows increase in strain; adjacent sensor shows no such increase.
08:54:41 a.m. - EOC2-4-0017/Flagstaff, Arizona: Video coverage begins. (+35.198-111.651)
08:54:45 a.m. - EOC2-4-0034/Reno, Nevada: Video coverage ends. (+39.53-119.813)
08:54:46 a.m. - MCC-FLIGHT: Four hyd return temps?"
MCC-MMACS: "To the left outboard and left inboard elevon."
MCC-FLIGHT: "OK, is there anything common to them? DSC (discrete signal conditioner) or MDM (multiplexer-demultiplexer) or anything? I mean, you're telling me you lost them all at exactly the same time?"
08:54:49 a.m. - EOC2-4-0026/Sparks, Nevada: Video coverage ends. (+39.541-119.768)
08:54:53 a.m. - EI+644 - Main landing gear left outboard wheel temperature begins off-nominal trend; two bit flips up. H=225,610; Mach: 22.22 (+37.933-116.896)
08:54:58 a.m. - MCC-MMACS: "No, not exactly. They were within probably four or five seconds of each other."
MCC-FLIGHT: "OK, where are those, where is that instrumentation located?
08:55:00 a.m. - EI+651 - Qbar = 34.5 psf; Mach 22.1; wing leading edge stagnation temperature = 2,900 degrees.
08:55:04-06 a.m. - EI+655/657 - Debris No. 7: Seventh report of debris leaving the orbiter. No evidence of RCS thruster firings.
08:55:05 a.m. - EOC2-4-0028/St. George, Utah: Video coverage begins. (+37.22-113.622)
08:55:08 a.m. - MCC-MMACS: "All four of them are located in the aft part of the left wing, right in front of the elevons, elevon actuators. And there is no commonality."
08:55:11 a.m. - EOC2-4-0009-B/Springfield, California: Video coverage ends. (+36.226-118.805)
08:55:11 a.m. - EOC2-04-0021/St. George, Utah: Video coverage begins. (+37.591-115.059)
08:55:12 a.m. - EI+663 - System 3 left main landing gear brake sidewall valve return line temperature (forward) begins trending up. H=224,546; Mach: 22.02 (+37.674-115.479)
08:55:17-19 a.m. - EI+668/670 - Debris No. 7A, seen just aft of the orbiter envelope.
08:55:18 a.m. - MCC-FLIGHT: "No commonality."
08:55:21 a.m. - EI+672 - Drag is recorded at 11 feet per second squared. Flight control system begins incorporating drag measurements to derive altitude for vehicle navigation. Nominal event. H=224,002; Mach: 21.92 (37.535-114.781)
08:55:21-25 a.m. - EI+672/676 - Debris No. 8: Eighth report of debris leaving the shuttle. No evidence of RCS thruster firings.
08:55:22-28 a.m. - EI+673/679 - Debris shower A; report of debris just aft of the orbiter envelope. During this four seconds, a luminescent section of plasma appears to contain a shower of small particles and larger, discrete pieces of debris, including Debris 8, 9 and 10.
08:55:23 a.m. - EOC2-4-0005/Ivins, Utah: Video coverage begins. (+37.169-113.679)
08:55:24-28 a.m. - EI+675/679 - Debris No. 9: Ninth report of debris leaving the shuttle; seen inside shower 7A. No evidence of RCS thruster firings.
08:55:25-29 a.m. - EI+676/680 - Debris No. 10: Tenth report of debris leaving the orbiter; seen inside shower 7A, well aft of orbiter envelop. No evidence of RCS thruster firings.
08:55:30 a.m. - EOC2-04-0050/St. George, Utah: Video coverage begins. (+37.591-115.059)
08:55:32 a.m. - EI+683 - Columbia crosses the Nevada-Utah state line. H=223,400; Mach: 21.8 (+37.4-114.1)
08:55:33-35 a.m. - EI+684/686 - S-band return link comm dropout (event 12); first drop out after antenna switch to upper right aft antenna; inconclusive if this is off nominal.
08:55:35-39 a.m. - EI+686/690 - Debris No. 11: Eleventh report of debris leaving the orbiter; appears in a secondary parallel plasma trail well aft of orbiter envelope; a second piece of debris is also seen. No evidence of RCS thruster firings.
08:55:36 a.m. - EI+687 - OEX: Main landing gear forward wall spar strain gauge V12G9049A shows a sudden drop, followed by a gradual increase until going erratic at EI+930.
08:55:38-40 a.m. - EI+689/691 - Debris No. 11A, seen just aft of orbiter.
08:55:38-42 a.m. - EI+689/693 - Debris No. 11B, seen at the head of a parallel plasma trail aft of orbiter envelope.
08:55:38 a.m. - MCC-Commentator: "Columbia continuing in a right bank, the wings angled 43 degrees, speed 15,000 miles per hour, altitude 43 miles, 2,090 miles to touchdown at the Kennedy Space Center targeted for runway three-three at Kennedy at present. Crossing the continental United States, now crossing above southern Nevada to the north of Las Vegas."
08:55:41 a.m. - EI+692 - Mid fuselage port sill longeron temperature at x1215 detects an unusually high increase, from 0 F/min to 2.9 F/min. H=222,821; Mach: 21.69 (+37.238-113.405)
08:55:42-46 a.m. - EI+693/697 - Debris No. 11C, seen in a parallel plasma trail well aft of orbiter envelope.
08:55:44-46 a.m. - EI+695/697 - Debris No. 12: Twelfth report of debris leaving the orbiter; event was preceded and followed by secondary plasma trails. No evidence of RCS thruster firings.
08:55:49 a.m. - Columbia moves into sunlight from orbital darkness. (+37.096-112.795)
08:55:54 a.m. - EOC2-04-0050/St. George, Utah: Video coverage ends. (+37.591-115.059)
08:55:54-58 a.m. - EI+705/708 - Debris No. 13: Thirteenth report of debris leaving the orbiter; event was followed by a brief brightening of the plasma trail adjacent to debris. No evidence of RCS thruster firings.
08:55:55 a.m. - EI-706 - Columbia crosses the Utah-Arizona state line. H=222,100; Mach: 21.5 (+37.0-112.4)
08:55:57 a.m. - EOC2-4-0030/Las Vegas, Nevada: Video coverage ends. (+36.309-115.274)
08:55:57-59 a.m. - EI+708/710 - Debris No. 14: Fourteenth report of debris leaving the orbiter; seen just aft of orbiter envelope. Debris 6 and 14 are visually the brightest debris events seen.
08:56:00-03 a.m. - EI+711/714 - S-band return link comm dropout (event 13); on upper right aft antenna; not clear if this is off nominal.
08:56:02 a.m. - EI+713 - Qbar = 40 psf. Aft reaction control system pitch jets are deactivated. Pitch control is now provided by elevator and body flap commands. H=221,670; Mach: 21.45 (+36.883-111.924)
08:56:02 a.m. - MCC-FLIGHT: "MMACS, tell me again which systems they're for."
MCC-MMACS: "That's all three hydraulic systems. It's... two of them are to the left outboard elevon and two of them to the left inboard.
08:56:03 a.m. - EI+714 - Left lower wing skin temperature begins trending down due to possible sensor or wiring damage. H=221,612; Mach: 21.44 (+36.866-111.858)
08:56:06 a.m. - EOC2-4-0028/St. George, Utah: Video coverage ends. (+37.767-115.972)
08:56:08-12 a.m. - EI+719/723 - Debris No. 15: Fifteenth report of debris leaving the orbiter; seen just aft of orbiter envelope. RCS thruster R2R fired briefly at 8:56:17 and :54 and R3R fired briefly at 8:56:17 and :52.
08:56:10 a.m. - EOC2-4-0005/Ivins, Utah: Video coverage ends. (+37.169-113.679)
08:56:12 a.m. - MCC-FLIGHT: "OK, I got you.
MCC-GNC: "Flight, guidance, we're processing drag with good residual."
MCC-FLIGHT: "Copy. Thank you."
08:56:16 a.m. - EI+727 - Hydraulic system 1 left main gear uplock actuator unlock line temperature increases from 0.7 F/min to 3.9 F/min; increases through LOS. H=220,778; Mach: 21.28 (+36.625-110.936)
08:56:17 a.m. - EI+728 - System 3 left main gear brake switch valve return line temperature (forward) sees an increase from 1.5 F/min to 8.8 F/min; remains constant to LOS. H=220,711; Mach: 21.27 (+36.607-110.871)
08:56:17 a.m. - EOC2-04-0021/St. George, Utah: Video coverage ends. (+37.591-115.059)
08:56:20 a.m. - EI+731 - Left main gear brake line temperature C sensor sees change from 1.3 F/min to 9.9 F/min; remains constant to LOS. H=220,488; Mach: 21.23 (36.554-110.676)
08:56:22 a.m. - EI+733 - Left main gear brake line temperature B sensor sees a rise rate change from 2.1 F/min to 9.1 F/min; continues increasing through LOS. H=220,374; mach: 21.21 (+36.518-110.546)
08:56:24 a.m. - EI+735 - Left upper wing skin temperature sensor sees start of off-nominal trend downward due to possible sensor or wiring damage). H=220,235; Mach: 21.17 (+36.482-110.417)
08:56:30 a.m. - EI+741 - Columbia begins the first of four banking maneuvers called roll reversals to bleed off energy. H=219,820; Mach: 21.13
08:56:39 a.m. - MCC-GC: "Flight, GC."
MCC-FLIGHT: "Go."
MCC-GC: "Your air-to-grounds are enabled for the landing count."
MCC-FLIGHT: "Thank you."
08:56:45 a.m. - EI+756 - Columbia crosses the Arizona-New Mexico state line. H=219,000; Mach: 20.9 (+36.1-109.0)
08:56:49 a.m. - MCC-Commentator: "Columbia's course continuing across Arizona and the Arizona and Mexico border near the four corners area of the United States. Its course will take it almost directly above Albuquerque, Mexico, it's altitude now 225,000 feet or 42 miles, speed 14,300 miles per hour, 1,785 miles to touchdown at the Kennedy Space Center.
08:56:53 a.m. - EI+764 - System 3 left main gear strut actuator temperature sees increase from 1.7 F/min to 12.9 F/min; remains constant through LOS. H=218,839; Mach: 20.80
08:56:55 a.m. - EI+766 - First roll reversal complete. H=218,817; Mach: 20.76
08:57:00 a.m. - EI+771 - Qbar = 42 psf; Mach 20.7; wing leading edge stagnation temperature = 2,900 degrees.
08:57:00 a.m. - EI+771 - Body flap deflected upward 3 degrees; considered nominal.
08:57:09 a.m. - EI+780 - OEX: Fuselage side surface temperature sensor V07T9270A starts off-nominal trend (rise, fall, rise).
08:57:09 a.m. - EI+780 - OEX: Fuselage lower surface temperature sensor V07T9508A begins an unusual trend (shallow drop).
08:57:11 a.m. - MCC-Commentator: It's banking now back to the left, the second in a series of four banks that dissipate speed of the spacecraft as it becomes an aircraft and descends into the atmosphere toward Florida. Wings angled about 75 degrees to the left."
08:57:19-29 a.m. - EI+790/800 - Debris No. 16. Very faint debris observed leaving the orbiter over eastern Arizona and New Mexico. Observations by observers at Kirtland AFB Starfire Optical Range; numerous jet firings inferred from injector temperatures.
08:57:19 a.m. - EI+790 - Main landing gear left outboard tire pressure 1 begins an off-nominal trend (bit flip up). H=217,757; Mach: 20.45 (+35.385-106.785)
08:57:24 a.m. - EI+795 - Main landing gear left outboard tire pressure 2 begins an off-nominal trend (bit flip up). H=217,315; Mach: 20.38 (+35.290-106.481)
08:57:25 a.m. - MCC-FLIGHT: "GNC, FLIGHT."
MCC-GNC: "FLIGHT, GNC."
MCC-FLIGHT: "Everything look good to you, control and rates and everything is nominal, right?"
08:57:28 a.m. - EI+799 - Left lower wing skin temperature drops off-scale low (sensor failure). H=216,845; Mach: 20.31 (+35.215-106.239)
08:57:31 a.m. - EOC2-4-0017/Flagstaff, Arizona: Video coverage ends. (+35.198-111.651)
08:57:35 a.m. - MCC-GNC: "Control's been stable through the rolls that we've done so far, flight. We have good trims. I don't see anything out of the ordinary."
08:57:43 a.m. - EI+814 - Left upper wing skin temperature sensor drops off-scale low. H=215,020; Mach: 20.09
08:57:45 a.m. - MCC-FLIGHT: "OK. And MMACS, FLIGHT?"
MCC-MMACS: "FLIGHT, MMACS."
MCC-FLIGHT: "All other indications for your hydraulic system indications are good."
08:57:53 a.m. - MCC-MMACS: "They're all good. We've had good quantities all the way across."
MCC-FLIGHT: "And the other temps are normal?"
MCC-MMACS: "The other temps are normal, yes sir."
08:57:53.5-55.5 a.m. - EI+824.5/826.5 - Flare No. 1: Asymmetrical brightening of orbiter shape over Mexico. Observed by Starfire Optical Range personnel. Numerous rocket firings.
08:57:54 a.m. - EI+825 - System 2 left brake switch valve return temperature (aft) begins seeing an off-nominal temperature increase. H=213,270; mach: 19.91
08:57:59 a.m. - MCC-FLIGHT: "And when you say you lost these, are you saying that they went to zero..."
MCC-MMACS: "All four of them are off-scale low."
MCC-FLIGHT: "... or off-scale low."
MCC-MMACS: "And they were all staggered. They were, like I said, within several seconds of each other."
MCC-FLIGHT: "OK."
08:57:59.5-58:01.5 a.m. - EI+830.5/832.5 - Flare 2: Asymmetrical brightening of orbiter shape over eastern Arizona and New Mexico. Observed by Starfire Optical Range personnel. Numerous rocket firings.
08:58:00 a.m. - EI+831 - Qbar = 52.5 psf; Mach 19.8; wing leading edge stagnation temperature = 2,880 degrees.
08:58:03 a.m. - EI+834 - Start of "sharp" elevon trim increase to counteract increasing aerodynamic drag (timing +/- 10 seconds). H=212,007; Mach: 19.79
08:58:04 a.m. - EI+835 - OEX: Left fuselage side surface temperature sensor V07T9253A begins unusual increase.
08:58:04-58:19 a.m. - EI+835/850 - Substantial increase in calculated rolling and yawing moments and initial indication of unusual pitching moment change.
08:58:16 a.m. - EI+847 - Left main gear brake line temperature sensor D sees a rise rate change from 0.9 F/min to 11.7 F/min (not increasing) to LOS. H=210,304; Mach: 19.55 (+34.287-103.293)
08:58:20 a.m. - EI+851 - Columbia crosses the New Mexico-Texas state line. H=209,800; Mach: 19.5 (+34.2-103.1)
08:58:32 a.m. - EI+863 - Main landing gear left outboard/inboard tire pressure 1 sensors see pressure trending down to off-scale low; main landing gear left outboard wheel temperature begins trending down to off-scale low (timing not exact; follows 7-second loss of signal)
08:58:32-59:22 a.m. - EI+863/913 - System 2 left brake switching valve return temperature (aft) sees rise from 2.5 F/min to 40 F/min until peak at 8:59:22 a.m. H=208,380; Mach: 19.28 (+33.980-102.325)
08:58:36 a.m. - EI+867 - Main landing gear inboard wheel temperature begins trending down to off-scale low. H =207,918; Mach: 19.21 (+33.908-102.099)
08:58:36 a.m. - MCC-Commentator: "Columbia continuing toward Florida, now approaching the Mexico-Texas border. Altitude 40 miles..."
08:58:38 a.m. - EI+869 - Main landing gear outboard tire pressure 1 sensor drops off-scale low.
08:58:39 a.m. - EI+870 - Main landing gear left outboard wheel temperature goes off-scale low; main landing gear left outboard tire pressure 2 sensor begins trending down to off-scale low. (+33.873-101.987)
08:58:40 a.m. - EI+871 - Columbia's backup flight system (BFS) computer displays tire pressure fault message on a cockpit display.
08:58:40 a.m. - EI+871 - Main landing gear inboard tire pressure 1 sensor drops off-scale low. H=207,370; Mach: 19.13 (+33.837-101.875)
08:58:41 a.m. - EI+872 - Main landing gear left inboard tire pressure 2 sensor stars off-nominal increase, rising about 3.5 psia in 2 seconds. H=207,132; Mach: 19.09
08:58:43 a.m. - EI+874 - Main landing gear inboard tire pressure 2 begins trending down.
08:58:44 a.m. - MCC-FDO: "FLIGHT, FDO."
08:58:48 a.m. - STS-CDR: "And, uh, Hou(ston)..."
08:58:48 a.m. - EI+879 - Main landing gear left inboard wheel temperature and main landing gear inboard tire pressure 2 sensors drop off-scale low. H=206,403; Mach: 18.99
08:58:51 a.m. - MCC-Commentator: "... speed 13,200 miles per hour. Range to touchdown 1,400 miles. The shuttle in a left bank with the wings banked about 57 degrees to horizontal."
08:58:54 a.m. - EI+885 - Main landing gear left outboard tire pressure 2 sensor drops off-scale low. H=205,553; Mach: 18.86
08:58:56 a.m. - EI+887 - Backup flight system computer displays tire pressure fault message (final message). H=205,311; Mach: 18.83 (+33.541-100.931)
08:59:00 a.m. - EI+891 - Qbar = 63.5 psf; Mach 18.7; wing leading edge stagnation temperature = 2,850 degrees.
08:59:06 a.m. - MCC-FLIGHT: "FDO, FLIGHT."
MCC-FDO: "Uh, we have the balloon. It is being run through DDS (data display system) right now."
08:59:06 a.m. - EI+897 - Left main gear downlocked indication - transferred ON - uplock indicates no change. H=204,336; Mach: 18.86 (+33.370-100.384)
08:59:09-39 a.m. - EI+900/930 - OEX: Several left-side temperature readings show a rapid increase followed by erratic behavior and loss of data around EI+940; includes six left OMS pod sensors and three left fuselage sidewall sensors.
08:59:15 a.m. - MCC-MMACS: "FLIGHT, MMACS."
MCC-FLIGHT: "Go."
08:59:18 a.m. - MCC-MMACS: "We just lost tire pressure on the left outboard and left inboard, both tires."
08:59:22 a.m. - EI+913 - System 2 left brake switching valve return temperature sensor (aft) begins a sharp downward trend to off-scale low.
08:59:23 a.m. - EI+914 - Loss of realtime data in mission control workstations.
08:59:24 a.m. - MCC-CAPCOM: "And Columbia, Houston, we see your tire pressure...
MCC-FLIGHT: "Copy..."
MCC-CAPCOM: "...messages and we did not..."
MCC-FLIGHT: "Is it instrumentation, MMACS? Gotta be..."
MCC-CAPCOM: "...copy your last."
08:59:26-28 a.m. - EI+917/919 - Sudden increase in rate of change of pitch, roll and yaw increments; magnitude begins to exceed the ability of the aileron to trim the vehicle.
08:59:30.66 a.m. - EI+921.66 - Start of R2R yaw jet firing; jets on at loss of signal to assist elevons in counteracting the increasing aerodynamic drag. H=200,767; Mach: 18.16 (+32.956-99.041)
08:59:30.68 a.m. - EI+921.68 - Start of R3R yaw jet firing; jet on at loss of signal to assist elevons in counteracting the increasing aerodynamic drag.
08:59:30 a.m. - MCC-MMACS: "FLIGHT, MMACS, those are...
08:59:31 a.m. - EI+922 - Maximum observed elevon deflections; Left: -8.11 degrees up; Right: -1.15 degrees up
MCC-MMACS: "...also off-scale low."
08:59:31.4 a.m. - EI+922.4 - Flight control system channel 4 aerosurface position measurements start trending toward their null values. This indicates worsening effects of wiring shorts.
08:59:31.478 a.m. - EI+922.5 - All flight control system channel 4 bypass valves close (indicate bypass). This is an indication of aerosurface actuator (ASA) high-rate data failure.
08:59:31.7 a.m. - EI+922.7 - Speedbrake channel 4 OI position measurement indicates 19, 20 and 24 degrees open over last three samples prior to loss of signal. Speedbrake should be closed at 0 degrees. No change seen in actuator motion. Signature considered nominal response to bypass valve closing (see above).
08:59:32 a.m. - EI+923 - Maximum observed elevon trim at LOS (-2.3 degrees).
08:59:32 a.m. - EI+923 - Columbia is approaching Dallas, Texas. Approximate location at initial loss of signal. H=200,700; Mach: 18.1 (+32.9-99.0)
08:59:32 a.m. - STS-CDR: "Roger, uh buh (CUTOFF)" (Editor's note: Phonetically, sounded like first syllable of "before" or possibly "both;" he may have been responding to the BFS fault messages for both left-side main landing gear tires)
08:59:32 a.m. - EI+923 - Loss of signal for left mid fuselage bondline temperature sensor at x1215; left aft fuselage sidewall temperature at x1410; left main gear brake line temperatures (A: 172.2 F; B: 154.2 F; C: 104.8 F; D: 88.3 F); left main gear strut actuator temperature (76.3 F); hydraulic system 1 left main gear uplock actuator unlock line temperature (52.2 F); System 2 left brake switch valve return temperature (aft, 62.8 F); system 3 left main gear brake switch valve return line temperature (67.3 F)
08:59:32.13 a.m. - EI+923.13 - Flight control system channel 4 fail flags raised on all aerosurface actuators.
08:59:32.136 a.m. - EI+923.136 - INITIAL LOSS OF SIGNAL - Last valid data frame accepted by ODRC - OI/BFS/PASS. The backup flight system computer selected the upper right aft quad antenna to communicate with TDRS-West. The pointing angle was off the shuttle's tail at -65 degrees and trending further into blockage; previous experience shows a probable loss of communications at angles greater than -60 degrees. Therefore, the loss of communications experienced here is consider normal and not the result of any failure or attitude change by the orbiter.
Editor's note: The following data was reconstructed based on a final two-second burst of telemetry beginning at 9:00:02.66 a.m.
08:59:32.195 a.m. - EI+923.195 - ASA 4 remote power controller and A&C trip indication due to electrical short.
08:59:33.598 a.m. - EI+923.598 - Left outboard bypass valve reopens. A "force fight" between channels 1/2/3/4 begins, resulting in a difference of up to 0.5 degrees between left outboard and inboard elevons; indicates a short in the bypass valve.
08:59:33.680 a.m. - EI+924.680 - Backup flight system fault message (1): Flight control system Channel 4 (TDRS-East data). Error is detected by ATVC/ASA hardware when sensed change in pressure across the actuator exceeds a limit indicating the FCS channel is no longer driving the actuator.
08:59:33.863 a.m. - EI+924.863 - PASS flight computers annunciate a fault (1): Flight control system channel 4 (TDRS-East data).
08:59:33.976 a.m. - EI+924.976 - Master alarm sounds in the cockpit.
08:59:34.518 a.m. - EI+925.518 - Left outboard "force fight" ends; driver currents go to zero, indicating remote power controller B has tripped; all bypass valves would open.
08:59:34.561 a.m. - EI+925.561 - Speed brake force fight begins and continues to LOS; indicates opening of all bypass valves due to RPC B trip on ASA 4. Speedbrake is already at zero.
08:59:35-36 a.m. - EI+926/927 - Vehicle sideslip changes sign. Just prior to initial LOS, the magnitude of Columbia's negative sideslip started to decrease; Between 8:59:34 and 8:59:37, sideslip grew from -.6 to +.8 degrees. Aerodynamic forces due to sideslip are now reinforcing the drag caused by problems with the left wing.
08:59:36 a.m. - EI+927 - Bank attitude error begins growing. Up until this moment, the flight control system had been able to maintain a bank angle error around 5 degrees. Aerojet DAP (digital autopilot) drops the left wing to compensate for increasing drag, creating a bank attitude error.
08:59:36.8 a.m. - EI+927.8 - Aerojet DAP commands a third RCS jet - R4R - to fire to counteract increasing aerodynamic forces pulling vehicle to the left (yaw down relative to Earth); R4R fires and remains on through 8:59:37.396 a.m. when data is lost for 25 seconds.
08:59:37 a.m. - Begin hypothetical trajectory plot for an object with a ballistic number = 220 psf. This trajectory is projected to compute an approximate impact point.
08:59:37.3 a.m. - EI+928.3 - Aerojet DAP orders R1R to begin firing; stays on through LOS at 8:59:37.396 a.m.
08:59:37.X a.m. - EI+928.X - Last aileron data; position now approximately -5.2 degrees with about -2.5 degrees of trim. Rate of change had reached maximum allowed by flight control system.
08:59:37.396 a.m. - EI+928.396 - Loss of data for 25 seconds. Additional data in this 25-second gap is recovered in computer buffers during the final two second burst of telemetry.
08:59:39-14:00:19 a.m. - EI+930/970 - OEX: Starting at 8:59:39 a.m., all OEX data becomes erratic.
08:59:46-48 a.m. - EI+937/939 - Debris A: Large debris seen leaving the orbiter, falling away from orbiter envelope.
08:59:46.347 a.m. - EI+937.347 - PASS flight computers generate a "roll reference" fault message. This message is recovered during final two seconds of telemetry in a computer buffer. The timing of this message - 10 seconds after four aft jets began firing - indicates rapid change in lift-to-drag ratio. BFS does not have this message in the fault message stack. It is likely the BFS annunciated this message during the 25-second LOS. If so, it was pushed out of the stack by at least five additional fault messages.
08:59:52.114 a.m. - EI+943.114 - PASS fault message: Left RCS leak; found in PASS fault message buffer (data suspect); indicates a leak of either helium and/or propellant; also possible this is due to erroneous temperature and pressure readings.
08:59:58 a.m. - MCC-INCO: "FLIGHT, INCO."
MCC-FLIGHT: "Go."
MCC-INCO: "Just taking a few hits here. We're right up on top of the tail. Not too bad."
08:59:59 a.m. - EOC2-4-0018/Duncanville, Texas: Video coverage begins. (+32.653-96.908)
09:00:00 a.m. - EOC2-4-0024/Arlington, Texas: Video coverage begins. (+32.736-97.108)
09:00:00 a.m. - EI+951 - Wing leading edge stagnation temperature = 2,800 degrees.
09:00:01-03 a.m. - EI+952/954 - Debris B seen well aft of orbiter envelope.
09:00:01.540 a.m. - EI+952.540 - BFS fault message: Left RCS leak; found in BFS fault message buffer (data, timing suspect).
09:00:01.9 a.m. - EI+952.9 - BFS fault message: Left RCS leak; found in BFS fault message buffer (data, timing suspect).
09:00:02-04 a.m. - EI+953/955 - Debris C - large piece - seen leaving the orbiter and falling away.
09:00:02.654 a.m. - EI+953.654 - BFS fault message: Left RCS LJET (data suspect). Message generated when left-side RCS jet fails OFF/ON/LEAK.
09:00:02.660 a.m. - EI+953.660 - Telemetry resumes for approximately two seconds after a 25-second drop out. Data from this final burst is suspect because of multiple bit errors. Only one data sample was available for many measurements. As a result, some of the following conclusions may be in error.
NOMINAL SYSTEMS: Columbia's APUs were running and the water spray boilers were providing cooling. The main propulsion system (aft engine compartment) was intact. The shuttle's electricity producing fuel cells were generating power and the fuel cell hydrogen/oxygen distribution lines were intact. Communications and navigation systems in the forward fuselage were performing normally. Rudder/speedbrake, body flap, main engine and right wing temperature sensors appeared active. The flash evaporator system had shut down. Life support systems were operating normally, although the flash evaporator cooling system was in shutdown.
OFF-NOMINAL SYSTEMS: All three hydraulic systems showed zero pressure and empty reservoirs. The left inboard and outboard elevon actuator temperatures were either off-scale low or show no data. The water spray boilers appeared to be over cooling the APU lubrication oil. The flash evaporator cooling system was in shutdown. The majority of the left orbital maneuvering system pod sensors were either off-scale low or showing no data. Multiple BFS and PASS fault messages for left OMS pod hardware were found in buffers (not enough data to determine if real leaks were present or if readings were due to loss of instrumentation). High temperatures at the bottom bondline centerline skin forward and aft of the wheel wells and at the port side structure over the left wing were seen. A general upward shift in main bus amps and downward shift in main bus volts was observed. AC3 phase A inverter appeared disconnected from the AC bus.
SHUTTLE ATTITUDE: Guidance and navigation data suggests Columbia was in an uncommanded orientation, or attitude, and was exhibiting uncontrolled rates of motion. Yaw rate was at sensor maximum of 20 degrees per second, suggesting a possible tumble to the left. Because Columbia was in a left bank at the time, a yaw to the left would have had the effect of dropping the nose toward Earth. Flight control mode was in AUTO, meaning the pilots never took over manual control (see below). At this point, it appears the forward, mid and aft fuselage, the right wing and right OMS pod were still intact.
09:00:03.470 a.m. - EI+954.470 - BFS fault message: Left OMS tank pressure; found in BFS fault buffer. Fault is annunciated when OMS oxidizer or fuel tanks show pressures out of limits high or low (data suspect).
09:00:0X.XXX a.m. - BFS fault message: Unknown (timing unclear).
09:00:0X.XXX a.m. - BFS fault message: SM1 AC VOLTS. Occurred after left OMS tank pressure message (time info corrupted). Error message indicates AC bus 3 phase A, B or C voltage is out of limits high or low.
09:00:03.637 a.m. - EI+954.637 - PASS fault message: Left RCS PVT (data suspect).
09:00:03.637 a.m. - EI+954.637 - PASS fault message: Digital autopilot downmode rotational hand controller. One of the two rotational hand controller "joysticks" is moved beyond a preset limit, either because one of the pilots bumped it or because one of the pilots made a brief attempt to take over manual control. Because of software timing issues, this event could have occurred as early as 9:00:01.717 a.m. Fault message corroborated by an initialization flag for the Aerojet DAP roll stick function. However, during this two-second period, rotational hand controller remained centered (in detent) and DAP remains in AUTO through loss of signal. Data is potentially error prone.
09:00:04.826 a.m. - EI+955.826 - Last identifiable OI downlink frame.
09:00:05.2-06.2 a.m. - EI+956.2/957.2 - Late flash 1; sudden brightening of the orbiter envelope.
09:00:06.2-07.2 a.m. - EI+957.2/958.2 - Late flash 2; sudden brightening followed by a shower of debris seen aft of orbiter over next four seconds.
09:00:08-12 a.m. - EI+959/963 - Debris D; seen slightly aft of orbiter envelope, generating its own tail.
09:00:09-13 a.m. - EI+960/964 - Debris E; seen aft of debris D.
09:00:10-14 a.m. - EI+961/965 - Debris F; first seen aft or orbiter; generates its own tail.
09:00:13-17 a.m. - EI+964/968 - Debris shower; multiple objects seen just aft of orbiter envelope over next two seconds.
09:00:13.439 a.m. - EI+964.439 - OEX: PCM (pulse code modulation) loss of synch; end of data.
09:00:18 a.m. - MCC-FLIGHT: "MMACS, FLIGHT."
09:00:17.8-18.8 a.m. - EI+968.8/969.8 - Catastrophic event of unknown nature; orbiter envelope suddenly brightens followed by dramatic change in the plasma trail. Presumed main body breakup.
09:00:19.44 a.m. - EI+970.44 - OEX: FDM (frequency division multiplexer) data ends. Prior to this moment, the fuselage was still intact and power was still flowing from Columbia's fuel cells.
09:00:21 a.m. - EOC2-4-0025/Camp Swift, Texas: Video coverage begins. (+30.191-97.292)
09:00:21-25 a.m. - Onset of vehicle main body breakup.
MCC-MMACS: "FLIGHT, MMACS."
MCC-FLIGHT: "And there's no commonality between all these tire pressure instrumentations and the hydraulic return instrumentations."
09:00:23 a.m. - EOC2-4-0024/Arlington, Texas: Video coverage ends. (+32.736-97.108)
09:00:27 a.m. - MCC-MMACS: "No sir, there's not. We've also lost the nose gear down talkback and the right main gear down talkback."
MCC-FLIGHT: "Nose gear and right main gear down talkbacks?"
MCC-MMACS: "Yes sir."
09:00:30 a.m. - Time-stamped video from Apache helicopters flying near Fort Hood, Texas, shows multiple contrails.
09:00:32 a.m. - RV2/Fort Hood, Texas: Video coverage begins. (+31.117-97.728)
09:00:35 a.m. - EOC2-4-0018/Duncanville, Texas: Video coverage ends. (+32.653-96.908)
09:00:51 a.m. - MCC-EECOM: "And FLIGHT, EECOM."
MCC-FLIGHT: "EECOM."
MCC-EECOM: "I've got four temperature sensors on the bond line data that are off-scale low."
09:00:53 a.m. - EI+1004 - End of peak heating region.
09:01:01 a.m. - EOC2-4-0025/Camp Swift, Texas: Video coverage ends. (+30.191-97.292)
09:01:16 a.m. - MCC-Commentator: "Columbia out of communications at present with mission control as it continues its course toward Florida..."
09:01:19 a.m. - RV2/Fort Hood, Texas: Video coverage ends. (+31.117-97.728)
09:01:29 a.m. - MCC-INCO: "FLIGHT, INCO, I didn't expect, uh, this bad of a hit on comm."
09:01:38 a.m. - MCC-FLIGHT: "GC, how far are we from UHF? Is that two-minute clock good?"
MCC-UNKNOWN: "Affirmative, FLIGHT."
09:02:00 a.m. - MCC-GNC: "FLIGHT, GNC."
MCC-FLIGHT: "Go."
MCC-GNC: "If we have any reason to suspect any sort of controllability issue, I would keep the control cards handy on page four-dash-13."
MCC-FLIGHT: "Copy."
09:02:21 a.m. - MCC-Commentator: "Fourteen minutes to touchdown for Columbia at the Kennedy Space Center. Flight controllers are continuing to stand by to regain communications with the spacecraft..."
09:02:29 a.m. - MCC-FLIGHT: "INCO, we were rolled left last data we had and you were expecting a little bit of ratty comm, but not this long?"
09:02:37 a.m. - MCC-INCO: "That's correct, FLIGHT. I expected it to be a little intermittent. And this is pretty solid right here."
MCC-FLIGHT: "No onboard system config changes right before we lost data?"
MCC-INCO: "That is correct, FLIGHT. All looked good."
MCC-FLIGHT: "Still on string two and everything looked good?"
MCC-INCO: "String two looking good."
09:03:03 a.m. - MCC-GC: "Two minutes to MILA."
09:03:12 a.m. - MCC-CAPCOM: "Columbia, Houston, comm check."
09:03:23 a.m. - MCC-FDO: "FLIGHT, FDO."
MCC-FLIGHT: "Go."
MCC-FDO: "Close-end aim point with the one-hour balloon shows us touching down at 1,496, 1,500 feet down the runway. Our crosswind right now is on the left, from the left on the three-three end."
09:03:34 a.m. - Reference trajectory ground impact in western Louisiana for hypothetical object with a ballistic number = 220 psf. (+30.781-92.557)
09:03:40 a.m. - MCC-CAPCOM: "Columbia, Houston, UHF comm check."
09:03:45 a.m. - MCC-Commentator: "CAPCOM Charlie Hobaugh calling Columbia on a UHF frequency as it approaches the Merritt Island tracking station range in Florida. Twelve-and-a-half minutes to touchdown, according to clocks in mission control." (listeners hear unease in the voice inflection)
09:03:46 a.m. - MCC-FDO: "FLIGHT, I'd like to stay where we're at."
MCC-FLIGHT: "I copy."
09:03:53 a.m. - MCC-MMACS: "FLIGHT, MMACS."
MCC-FLIGHT: "MMACS?"
MCC-MMACS: "On the tire pressures, we did see them go erratic for a little bit before they went away, so I do believe it's instrumentation."
MCC-FLIGHT: "OK."
09:04:05 a.m. - MCC-CAPCOM: "Columbia, Houston, UHF comm check."
09:04:35 a.m. - MCC-FDO: "FLIGHT, FDO."
MCC-FLIGHT: "Go."
MCC-MALE VOICE: "I know this data's a little late, the one-hour balloon protects us for winds...
09:04:41 a.m. - MCC-CAPCOM: "Columbia, Houston, UHF comm check."
MCC-FDO: "...I think we're in a smaller wind persistence case than that. In other words, we shouldn't expect as big of a change. I'm comfortable with 1,500 feet down the runway."
09:04:54 a.m. - MCC-Commentator: "Flight controllers are standing by for Columbia to move within communications range of the Merritt Island tracking station in Florida to regain communications with Columbia."
09:04:57 a.m. - MCC-GC: "Flight, GC."
MCC-FLIGHT: "Go."
MCC-GC: "MILA not reporting any RF at this time."
MCC-INCO: "FLIGHT, INCO, SPC just should have taken us to STDN low."
MCC-FLIGHT: "OK."
09:05:13 a.m. - MCC-FLIGHT: "FDO, when are you expecting tracking?"
MCC-FDO: "One minute ago, FLIGHT."
09:05:21 a.m. - MCC-Commentator: "Also, flight controllers standing by for tracking data of Columbia that's also received through the Merritt Island tracking station."
09:05:26 a.m. - MCC-CAPCOM: "Columbia, Houston, UHF comm check."
09:05:51 a.m. - MCC-Commentator: "Ten and a half minutes to anticipated touchdown for Columbia." (voice inflection signals uncertainty)
09:06:29 a.m. - MCC-GC: "And FLIGHT, GC, no C-band yet."
MCC-FLIGHT: "Copy."
09:06:56 a.m. - MCC-Commentator: "Flight controllers are still standing by for C-band tracking data from the Merritt Island tracking station of Columbia and UHF communications."
09:07:08 a.m. - MCC-CAPCOM: "Columbia, Houston, UHF comm check."
09:07:22 a.m. - MCC-INCO: "FLIGHT, INCO."
MCC-FLIGHT: "Go."
MCC-INCO: "I could swap strings in the blind."
09:07:36 a.m. - MCC-FLIGHT: "OK, command us over."
MCC-INCO: "In work, FLIGHT."
09:08:07 a.m. - MCC-Commentator: "Eight minutes on the touchdown clock for Columbia, flight controllers continuing to stand by to regain communications with the spacecraft."
09:08:25 a.m. - MCC-INCO: "FLIGHT, INCO, I've commanded string one in the blind."
MCC-FLIGHT: "INCO?"
MCC-INCO: "I've commanded string one in the blind, FLIGHT."
MCC-FLIGHT: "Copy."
09:08:34 a.m. - MCC-Commentator: "Flight controllers standing by for communications through the Merritt Island tracking station, a ground tracking site in Florida."
09:09:27 a.m. - MCC-GC: "And FLIGHT, GC."
MCC-FLIGHT: "Go."
MCC-GC: "MILA's taking one of their antennas off into a search mode."
MCC-FLIGHT: "Copy. FDO, FLIGHT?"
MCC-FDO: "Go ahead, FLIGHT."
MCC-FLIGHT: "Did we get, have we gotten any tracking data?"
MCC-FDO: "We got a blip of tracking data, it was a bad data point, FLIGHT. We do not believe that was the orbiter. We're entering a search pattern with our C-bands at this time. We do not have any valid data at this time."
09:09:29 a.m. - Projected time Columbia's velocity would have dropped to Mach 2.5 had this been a normal approach.
09:09:55 a.m. - MCC-FLIGHT: "OK. Any other trackers that we can go to?"
MCC-FDO: "Let me start talking, FLIGHT, to my navigator."
09:10:07 a.m. - MCC-Commentator: "This is mission control, Houston. Flight controllers are continuing to seek tracking data of Columbia. Touchdown clocks countdown to six minutes to touchdown for the anticipated shutdown, touchdown of Columbia at the Kennedy Space Center runway. Tracking data is being sought through the Merritt Island tracking station located near the Kennedy Space Center in Florida."
09:10:35 a.m. - MCC-Commentator: "Communications with Columbia were lost at about 8 a.m. Central time, about 10 minutes ago."
09:11:38 a.m. - Projected time Columbia's velocity would have dropped below the speed of sound had this been a normal approach.
09:12:34 a.m. - MCC-Commentator: "This is mission control, Houston. Flight controllers are continuing to stand by for communications from Columbia. The last communications with the spacecraft occurred about 8 a.m. Central time as it was above central Texas. Currently seeking communications or tracking data from the spacecraft through C-band radar and ground tracking sites located at the Merritt Island tracking station in Florida."
09:12:39 a.m. - Projected time Columbia would have been banking on the heading alignment cylinder to line up on runway 33 had this been a normal approach.
09:12:40 a.m. - (time approximate) Mission operations representative Phil Engelauf, sitting directly behind Cain, gets a call informing him that multiple contrails have been sighted along Columbia's path. This is the first notification of vehicle breakup in mission control, but it is not based on hard data. Engelauf tells Cain about the report. The flight director pauses a moment, digesting this, and then turns back to the flight control team to declare a contingency.
09:12:55 a.m. - MCC-FLIGHT: "GC, FLIGHT. GC, FLIGHT."'
MCC-GC: "FLIGHT, GC."
MCC-FLIGHT: "Lock the doors."
MCC-GC: "Copy."
09:13:17 a.m. - MCC-FLIGHT: "FDO, do you have any tracking?"
MCC-FDO: "No sir."
09:13:43 a.m. - MCC-MOD: "FLIGHT, MOD, on the flight loop."
09:13:51 a.m. - MCC-FDO: "FLIGHT, FDO."
MCC-FLIGHT: "Go."
MCC-FDO: "My C-bands have not acquired anything. We are only in track, uh, acquiring false locks at this time."
09:14:11 a.m. - MCC-FLIGHT: "I copy, FDO."
09:14:26 a.m. - MCC-Commentator: "This is mission control, Houston. Flight controllers continue to seek tracking or communications with Columbia through Merritt Island tracking station. Last communications with Columbia was at 8 a.m. Central time, approximately above Texas as it approached the Kennedy Space Center for its landing. Flight director LeRoy Cain is now instructing controllers to get out their contingency procedures and begin to follow those."
09:14:29 a.m. - MCC-FLIGHT: "OK, all flight controllers on the flight loop, we need to kick off the FCOH (Flight Control Operations Handbook) contingency plan procedure, FCOH checklist page 2.8-5."
09:14:52 a.m. - MCC-FLIGHT: "FDO, FLIGHT. ... FDO, FLIGHT."
MCC-FDO: "Go ahead."
MCC-FLIGHT: "Do you have any information or reports from Space Command?"
09:15:04 a.m. - MCC-Commentator: "Flight dynamics officer reports no tracking data from the C-band radar at the Merritt Island tracking station has been reported of any objects."
09:15:50 a.m. - Columbia's scheduled touchdown time on runway 33 at the Kennedy Space Center.
09:17:57 a.m. - MCC-FLIGHT "OK, all flight controllers, on page 9, of the FCOH procedure you need to make sure you step through the actions required in step 20, that's for your workstation logs, display printouts, there's a whole list of data collection items we need to make sure we log through."
09:18:20 a.m. - MCC-Commentator: "This is mission control, Houston. Flight director LeRoy Cain is instructing controllers to follow contingency procedures. The last communications with the shuttle Columbia during its descent from orbit were at about 8 a.m. Central time as it was descending through the atmosphere..."
09:18:36 a.m. - MCC-FLIGHT: "And GC, FLIGHT?"
MCC-GC: "FLIGHT, GC."
MCC-FDO: "FDO, FLIGHT
MCC-FLIGHT: "We need to take the equivalent of a command server TSU (Trajectory Server Upgrade) checkpoint..."'
MCC-FDO: "Yes sir."
MCC-GC: "Copy."
MCC-FLIGHT: "We don't have the old DSC (Dynamic Standby Computer) checkpoint but we have the equivalent capability that we need to do."
MCC-GC: "We'll get that done."
09:18:40 a.m. - MCC-Commentator: "...at an altitude of about 207,000 feet en route to the Kennedy Space Center in Florida and a touchdown that was anticipated to occur about two-and-a-half minutes ago. Flight controllers received no further communications with the spacecraft after about 8 a.m. Central time and no further tracking data from the spacecraft was gained from C-band tracking radar at the Merritt Island tracking station in Florida."
09:18:58 a.m. - MCC-FLIGHT: "GC, FLIGHT."
MCC-GC: "FLIGHT, GC."'
MCC-FLIGHT: "You understand how to do the end-of-file log tapes we need...
MCC-GC: "Yes sir."
MCC-FLIGHT: "...in the checklist? OK."
09:19:14 a.m. - MCC-Commentator: "Contingency procedures in effect in mission control require all operators to conserve all their data and logbooks and notes that have been taken, that being instructed by flight director LeRoy Cain for controllers to begin following those steps and secure all information."
09:19:34 a.m. - MCC-FLIGHT: "And folks, listen up again on the flight loop. No phone calls off site outside of this room, our discussions are on these loops, the recorded DVIS (digital voice integrated system) loops only, no data, no phone calls, no transmissions anywhere, into or out."

Columbia's crew
Blue shirts (left to right): David
Brown, Willie McCool, Michael Anderson
Red shirts (left to right): Kalpana
Chawla, Rick Husband, Laurel Clark, Ilan Ramon
MCC-GC: "FLIGHT, GC."
MCC-FLIGHT: "GC."
MCC-GC: "We have no way of disabling the black phones."
MCC-FLIGHT: "I understand."
09:20:10 a.m. - MCC-Commentator: "Again, flight director LeRoy Cain has declared a contingency. Flight controllers here in mission control are securing all their information, notes and data gathered from the spacecraft. The last communications with Columbia at 8 a.m. Central time as it was descending toward Florida for its landing. At that time, about 207,000 feet above central Texas traveling approximately 12,500 miles per hour, 1,192 miles from its touchdown at Kennedy Space Center. Since 8 a.m., no communications were received with Columbia and no tracking data received through the Merritt Island tracking station, those efforts made. The flight dynamics officer reports no objects tracked through that tracking data."