
Search continues for Auburn University student missing in Japan
James "Weston" Higginbotham, an Auburn University student, went missing last week in Japan after his family says he went to an area near Kyoto known for its hiking trails.
Watch CBS News
Weeknights 6:30PM ET on CBS
10PM ET on the CBS News app
James "Weston" Higginbotham, an Auburn University student, went missing last week in Japan after his family says he went to an area near Kyoto known for its hiking trails.

According to an official familiar with the investigation, new digital forensic evidence appears to undercut Brian Hooker's account of his wife's disappearance, although they did not specify how.

Former Shelby County police officer Karson Hyder has been charged with one count of assault inflicting serious injury after video appeared to show him repeatedly punching a woman.

The FLEX Rover will be equipped to carry two astronauts and traverse hundreds of miles of lunar terrain.

"You come first," declares the new anchor of the Evening News. "Not advertisers. Not politicians. Not corporate interests — including the new owners of CBS."
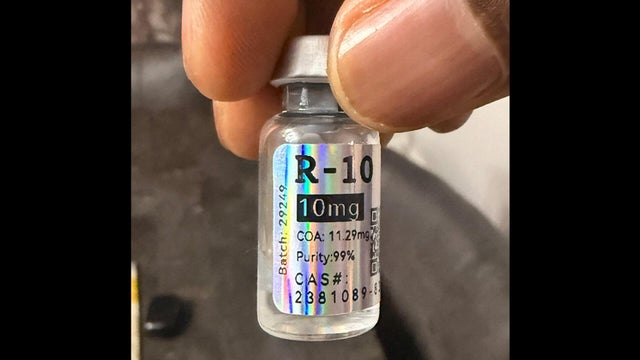
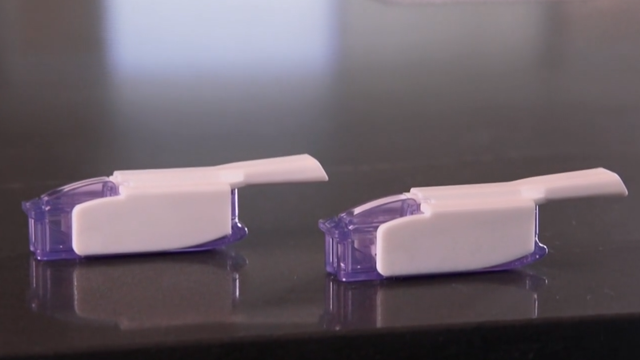
There's a new safety concern about doctors prescribing one experimental weight loss treatment, retatrutide, that hasn't even been FDA approved yet. Adam Yamaguchi reports.

Apple on Monday announced new safety features for kids and parents, changing how they will use their devices. Jo Ling Kent reports.

A man appeared in a Houston courtroom Monday after he was removed from a United Airlines flight last month for allegedly getting on the plane with a fake boarding pass. Jason Allen reports.

A powerful 7.8 magnitude earthquake rattled the Philippines early Monday local time, killing at least 35 people and injuring more than 200. Anna Coren has the latest.

President Trump urged both Israel and Iran to immediately stop attacking other Monday after an exchange of strikes on Sunday. The president insists that final negotiations for peace are ongoing, subject to what he called "ignorance or stupidity" getting in the way. Charlie D'Agata reports.
Nearly 90 million Americans are facing flood threats Monday night after rain during the day unleashed flash floods in Missouri, Arkansas, Kansas, Oklahoma and Texas. On top of that, heat alerts are also posted across the central plains with triple-digit heat moving in and pushing to the east by the end of the week. Meteorologist Rob Marciano is tracking it all.

President Trump will watch the New York Knicks and San Antonio Spurs in Game 3 of the NBA Finals from an executive suite, as an invited guest of Madison Square Garden CEO James Dolan. Ed O'Keefe reports.

It's part military jeep, part rolling art museum, and for Filipino Americans, it's a symbol of cultural identity and resilience. Itay Hod takes a ride on San Francisco's last jeepney.

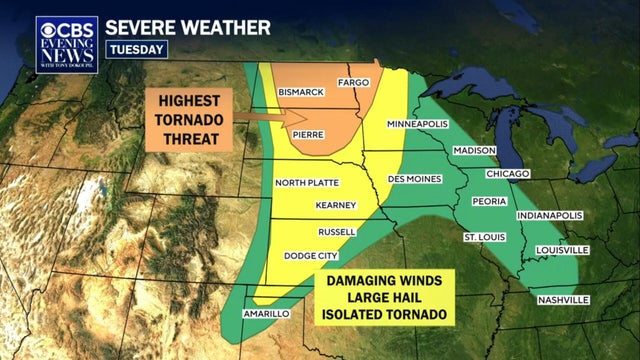
Millions in central U.S. facing severe weather threats after weekend of storms; Inside Trump's visit to the NBA Finals.

Iran strikes Israel for first time since April ceasefire in retaliation for Israeli attack on Beirut; 12 hurt in "gunfight" at Ohio festival, police say.

For more than five decades, St. Benedict's Preparatory School in Newark, New Jersey, has required its freshmen to go on a mandatory five-day, 55-mile hike on the Appalachian Trail. Steve Hartman explains why in "On the Road."

Steve Hartman goes "On the Road," following the story of a dog who was left at a Fort Worth, Texas, firehouse.

Schools teach kids how to read, write and do math. But what about a class on how to be kind? In some places, it is. Steve Hartman goes "On the Road" with the story.

58-year-old David White retired after 33 years in education, the last 15 spent as an elementary school principal in Atlanta. But after "just hanging out with the cat," he decided to go back to school as a handyman. Steve Hartman goes "On the Road" with the story.

Twenty-six-year-old Ana Duarte said that as a child, she and her mother were homeless in Florida. Now, she has found an apartment for her and her mom. Steve Hartman has the story.

The largest wildfire in Nebraska history burned about a thousand square miles of ranchland, including the Wintz's entire 11,000-acre ranch. When they and others faced the threat of losing their livelihoods, thousands of anonymous donors stepped up from across the U.S.

Nine-year-old Hayden Stine was born without most of her right arm. When she went to a Denver Summit women's soccer home opener, she saw a player, Carson Pickett, just like her. Steve Hartman goes "On the Road" with a story about the importance of role models.

George Strausman of Great Neck, New York, is 102 years old and still works four days a week in his family's construction business. But it's what he does on his day off that is even more remarkable. Steve Hartman has his story in "On the Road."

A girls' basketball team appealed their victory after the coach discovered they didn't actually win. Now, they're being lauded for their character. Steve Hartman has the update.

Federal immigration authorities barred a Somali soccer referee who was slated to officiate the FIFA World Cup from entering the U.S. over the weekend, citing "vetting concerns."

"The people are there to see these two teams play," Bill Bradley said of President Trump's plan to attend Game 3 of the NBA Finals on Monday night.
Going public will allow OpenAI, valued at $852 billion, to inject more cash into its business as the AI race quickens.

SpaceX is setting aside a large chunk of shares for ordinary investors as it seeks to raise a record $75 billion. Here's what to know.

"AI can make everything that was on my plate visible to colleagues while I'm gone," one expert said.
Going public will allow OpenAI, valued at $852 billion, to inject more cash into its business as the AI race quickens.
SpaceX is setting aside a large chunk of shares for ordinary investors as it seeks to raise a record $75 billion. Here's what to know.
"AI can make everything that was on my plate visible to colleagues while I'm gone," one expert said.

New York Fed survey shows growing concern about household finances and the job market, even as the job market remains solid.

Although working remotely offers flexibility, it also takes a toll on people's mental health, experts said.

Embattled International Criminal Court chief prosecutor Karim Khan was suspended after the court's oversight body referred him for disciplinary proceedings.

Donald Trump was booed loudly by fans inside Madison Square Garden when he was shown on video screens during the national anthem prior to Game 3 of the NBA Finals on Monday.

CBS News projects that incumbent Los Angeles Mayor Karen Bass will face off against Nithya Raman in November's runoff election.
Federal immigration authorities barred a Somali soccer referee who was slated to officiate the FIFA World Cup from entering the U.S. over the weekend, citing "vetting concerns."
"The people are there to see these two teams play," Bill Bradley said of President Trump's plan to attend Game 3 of the NBA Finals on Monday night.
There's a new safety concern about doctors prescribing one experimental weight loss treatment, retatrutide, that hasn't even been FDA approved yet. Adam Yamaguchi reports.

Doctors are jumping the gun to prescribe a medication lacking FDA approval that has gone viral on social media. "Why are we waiting?" one physician asked.
Approved 20 years ago as a diabetes treatment, GLP-1 drugs have been found to help patients reduce weight, changing the lives of more than 30 million people in the U.S. But there also have been troubling side effects reported.

Approved 20 years ago as a treatment for diabetes, GLP-1 drugs have been found also to help patients significantly reduce weight. More than 30 million people in the U.S. have had their lives changed by GLP-1 medications. But there have also been troubling side effects reported. Correspondent Tracy Smith talks with experts who say the drugs might prove useful in treating other diseases associated with obesity (including cancer); and with patients who have taken GLP-1 drugs and experienced widely varying reactions.
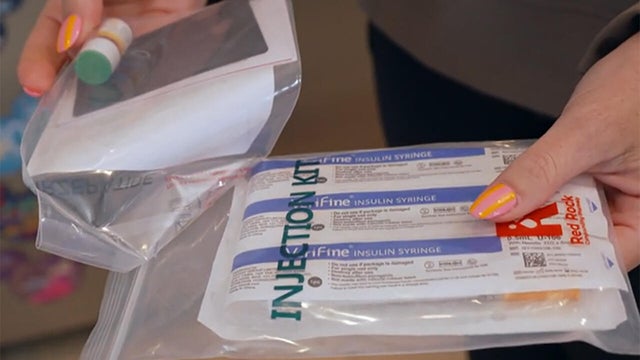
A medical breakthrough is showing promise for millions of Americans with Type 1 diabetes. It's an alternative to taking insulin without the injections. Mark Strassmann has more details.
Embattled International Criminal Court chief prosecutor Karim Khan was suspended after the court's oversight body referred him for disciplinary proceedings.

Great white sharks are classified as "critically endangered" in the Mediterranean Sea, and underwater sightings are incredibly rare.

Russia sanctioned Alexander Browder, son of financier-turned-activist Bill Browder, after he unveiled an alleged cryptocurrency money laundering network.

Pope Leo XIV denounced the "scourge" of sexual violence by Catholic clergy and called for a "culture of care" in the Church ahead of an expected private meeting with victims in Spain.

Iran and Israel declare a halt to fighting as President Trump says both are seeking an "immediate ceasefire" after a major escalation in the 101-day war.

Garry Nolan, a professor of pathology at Stanford University School of Medicine and the executive director of the board for The Sol Foundation, joins CBS News 24/7 to discuss Steven Spielberg's new movie, "Disclosure Day," and its exploration of the existence of aliens on Earth.

CBS News New York's Dave Carlin breaks down the biggest wins and performances from the 79th Tony Awards.
Oscar-winning director Steven Spielberg talks to CBS News about his 34th feature film, "Disclosure Day," which explores what would happen if all of the evidence about UFOs and alien life was released to the entire world and proved we are not alone. He also discusses his opinion on aliens, saying they "have been here and they are here."

At Broadway's biggest night, "Schmigadoon!" took home the award for best musical. Meanwhile, "Arthur Miller's 'Death of a Salesman'" won six Tony Awards, the most of the night. Jamie Wax has more on the winners and top moments.

"Schmigadoon!" — which was tied for the most nominations, with 12 — won Best Musical, and "Liberation" took home the honor of Best Play at the 2026 Tony Awards.
SpaceX is setting aside a large chunk of shares for ordinary investors as it seeks to raise a record $75 billion. Here's what to know.
"AI can make everything that was on my plate visible to colleagues while I'm gone," one expert said.

From labor shortages to environmental impacts, farmers are looking to AI to help revolutionize the agriculture industry. One California startup, Farm-ng, is tapping into the power of AI and robotics to perform a wide range of tasks, including seeding, weeding and harvesting.

LinkedIn's latest workforce report found hiring rates are nearly 5% lower than a year ago. Catherine Fisher, a LinkedIn career expert, explains how job applicants can break through the market, using AI when applying and more.

Prediction markets have become a draw for young men in search of quick cash and thrills, experts say. "I had almost $4,600 at one point but squandered that," one man said.
Great white sharks are classified as "critically endangered" in the Mediterranean Sea, and underwater sightings are incredibly rare.

The expected arrival of El Niño this summer could trigger another mass coral bleaching event, which would be the fifth on record, researchers said.

More than 5,300 years ago, Oetzi the Iceman was strolling through the Alps on the border of Austria and Italy when he was killed by an arrow in the back.

Days after a meteor exploded over New England, another fireball was spotted, visible in the Midwest to the Northeast. Rob Marciano has more.
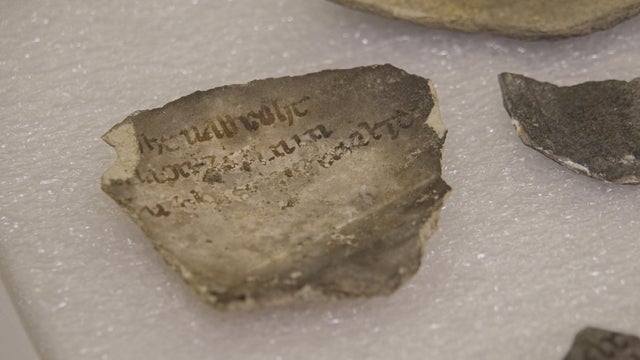
A team of archaeologists at the iconic cathedral is digging straight down and back in time, to Roman Paris 2,000 years ago.
A man appeared in a Houston courtroom Monday after he was removed from a United Airlines flight last month for allegedly getting on the plane with a fake boarding pass. Jason Allen reports.

At least 12 people were injured during a mass shooting at the Old West End Festival in Toledo, Ohio, officials say. CBS News' Jonah Kaplan reports.

Twelve people were injured, two of them critically, in what police are calling a "gunfight" that broke out at the Old West End Festival in Toledo, Ohio, on Saturday. Jonah Kaplan reports.

Six people, including the suspect, were taken to the hospital after a stabbing incident at New York City's Penn Station on Sunday evening.

A toxic couple orchestrates an elaborate plan to kill a mother. "48 Hours" correspondent Peter Van Sant reports.

Out of an abundance of caution, NASA briefly directed five of the seven crew members aboard the International Space Station to wait inside the docked SpaceX Crew Dragon "Freedom" spacecraft.
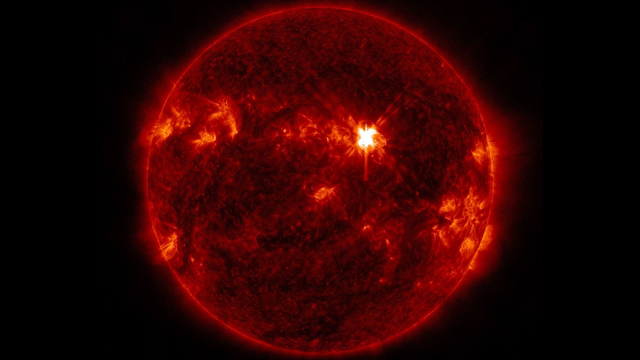
Three solar flares burst from the sun this week, raising the chances of seeing the northern lights for people across the United States.
NASA officials said the $582 million MAVEN orbiter could not be recovered after a problem on the far side of Mars late last year, and that its extraordinarily successful mission was at an end.

Damage to Blue Origin's lone launch pad in the wake of last week's spectacular explosion was not as severe as initially feared, the company said.
The FLEX Rover will be equipped to carry two astronauts and traverse hundreds of miles of lunar terrain.

A look back at the esteemed personalities who've left us this year, who'd touched us with their innovation, creativity and humanity.

Summer is the time to enjoy live music, indoors and out. Scroll through our gallery of some of 2026's leading musical acts, featuring images by CBS News photojournalist Jake Barlow and photographers Ed Spinelli and Kirstine Walton.

Does the evidence show a cover-up, or was Todd Kendhammer wrongfully convicted for the murder of his wife?

Family seeks answers in death of newlywed who disappeared in 2005 while on Mediterranean honeymoon cruise.

Meet the tattooed beauty charged in the death of Google executive Forrest Hayes.

Wisconsin state representative and self-described democratic socialist Francesca Hong launched what many would consider a long-shot candidacy for Wisconsin governor last year. But early polls show her as one of the frontrunners ahead of the Democratic primary on August 11. Hong joined CBS News to discuss her campaign.

Apple unveiled new child safety features for its devices at its annual Worldwide Developers Conference in Cupertino, California, Monday. CBS News senior business and tech correspondent Jo Ling Kent has more.

The Trump administration says it is moving forward with what it calls the largest-ever effort to use its power to revoke U.S. citizenship. CBS News immigration correspondent Camilo Montoya-Galvez has more.

Iran and Israel say they've halted military operations after weekend flare-up; Trump attends NBA Finals game at Madison Square Garden.
Millions in central U.S. facing severe weather threats after weekend of storms; Inside Trump's visit to the NBA Finals.